Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
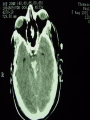
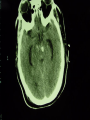
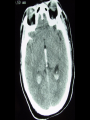
Altered Mental Status and Coma Brian Nelson Case No. 1 A 21 yo BF presents to the Baltimore City Hospital E.D. in the summer of ‘78. Her family states she is having a bad headache and needs her “Quiet World” tablets Case continues No history other than an Ambulance took her to another hospital earlier that day when a neighbor heard her screaming and called EMS At the other hospital an exam and CBC were said to be normal and she was discharged General Exam Patient grossly delirious, oriented to name only BP 125/70, P 76, RR 24, T 100.2 orally HEENT: PERRL, fundi difficult to evauate because of roaming eyes, grossly normal Neck: Very Stiff Chest: Loud wet rales throughout lung fields Neurologic Exam Able to follow only simplest comands, Cranial Nerves grossly intact, Cerebellar could not be tested, specific muslce group strength could not be tested, but patient moved all extremities and fought attempts to test range of motion. Reflexes, gait and Romberg could not be tested Diagnostic workup CXR: Complete opacification of left lung CBC: Hct 43, WBC 10.7 K, 75 segs, 17 bands, 7 lymphs ABGs on room air: 7.42/37/98 Lytes, BUN, glucose, Ca, PO4 all normal Provisional Diagnosis? Diagnosis and Dilemma Provisonal Diagnosis: Pneumococcal Pneumonia with secondary meningitis Plan? Allow that in 1978 the nearest CT scanner was 5 miles away (and slow first generation). Minimum time to get a head CT 3 hours LP was performed Opening pressure was 28 cm H2O 5 cc clear spinal fluid removed 5 minutes later the patient lost consciousness, dilated her left pupil and stopped breathing Coma mnemonic for the brain impaired Doc A for alcoholism E for encephalopathy I for insulin O for opiates U for uremia T for trauma and environmental disturbance I for infection P for psychiatric S for syncope Alcoholics have many reasons to be impaired Head trauma, hypothermia Infections: pneumonia, meningitis, sepsis Withdrawal: delerium tremens, post-ictal Metabolic: alcoholic ketoacidosis, lactic acidosis Brain atrophy, Wernicke’s, Korsakoff’s, lead encephalopathy Toxic alcohols: methanol, isopropyl, ethylene glycol Liver failure, hypoxia E for encephalopathy Post-ictal Hypertensive Encephalopathy Intracerebral mass CVA - vasocclusive • thrombosis • embolism • venous infarct CVA- hemorrhagic • Intracerebral hemorrhage • Subarachnoid hemorrhage I for insulin Too little • Diabetic Ketoacidosis • Hyperosmolar Non-ketotic Coma Too much • Hypoglycemia O for opiates Essentially any chemical including water sedatives anticholinergics hallucinogens sympathomimetics U for uremia Hyper and hypo Na, hyper and hypo Ca, hyper and hypo Mg, hypophosphatemia Hyper and hypo T4, Hyper and hypo adrenal, panhypopituitarism Liver, renal, and exocrine pancreas failure, HYPERCARBIA HYPOXIA, HYPOXIA, HYPOXIA T for trauma and environmental disturbance Epidural, Subdural, Subarachnoid and intracerebral hemorrhage Concussion and contusion Hypo and hyperthermia I for infection Meningitis Sepsis Brain abscess Encephalitis The weirdos: cerebral syphillis, malaria, tuberculosis, cystocercosis, nagleria, cryptococcosis, toxoplasmosis, etc P for psychiatric Hysteria Malingering Catatonia S is for syncope Arrhythmias Infarction Hypovolemia Hemorrhage Vasodepressor syncope Causes of Stupor or Coma in 500 patients Diffuse dysfunction 76% Supratentorial lesions 20% Subtentorial lesions 12% Psychiatric 8% Things that aren’t coma Dementia Acute Confusional State (Delerium) Persistent Vegetative State Akinetic Mutism Locked in syndrome Psychogenic Unresponsiveness Brain death When altered but not Coma, check components of consciousness Wakefulness Attention Working Memory Perception Long-term Memory Motivation Cognition Purposeful motor response Initial actions Check SaO2 and pupils, support respiration and oxygenation, Narcan for suspected narcotics OD Check BP and conjunctiva, treat shock and anemia Glucometer, admin glucose if indicated Two minute exam, Is it structural? History Pupillary reactions Oculocaloric respones Respiratory pattern Motor responses Skeletal tone Should have 95% accuracy of structural vs diffuse dysfunction Is it structural: History Sudden vs. gradual onset PMH: particulary depression, Diabetes, Drug user, medications prescribed or missing Is it structural: pupillary reactions Metabolic: small reactive Diencephalic: small reactive Midbrain: midposition, fixed CN III: unilateral dilated Pons: pinpoint fixed Medulla: dilated, fixed Tox: narcotics -pinpoint reactive, hypoxic, barbs - dilated and fixed Oculocalorics Brainstem intact: deviates to cold water Brainstem damaged: anything else Low brainstem: no response COWS is backwards, patient must have live vestibule, no vestibular toxic drugs Respiratory Pattern Eupnea: diffuse dysfunction Cheynes-Stokes: Diencephalon Sustained hyperventilation: Midbrain Ataxic: Medullary Motor Responses and tone Diffuse: aversive reactions Early diencephalon: aversive & cogwheeling Low diencephalon: flaccid or decorticate, tone decreased Midbrain: flaccid or decerebrate Medulla: lower extremity flexion Diffuse dysfunction Pupils small and reactive Oculocalorics: tonic deviation Tone: normal No posturing, normal tone Normal breathing of Cheyne-Stokes Psychogenic unresponsiveness Eyelids flutter and close actively Pupils small and reactive Tone variable, bizarre posturing may be present Optokinetic testing positive Oculocalorics: fast component present Supratentorial Mass Initially focal signs (the mass) Signs move rostral to caudal Signs point to one level at any time motor signs may be asymmetrical Supratentorial herniation Central Uncal Combined Early diencephalic phase Eupnea Pupils small and reactive conjugate deviation aversive motions cogwheeling (paratonia) Late diencephalic Cheyne-Stokes breathing Pupils small and reactive Conjugate deviation: easier less cortical control Flaccid or decorticate Mid-brain upper pons Sustained hyperventilation pupils mid position, fixed irregular oculocalorics impaired, dysconjugate flaccid or decerbrate Lower pons, upper medulla Ataxic breathing pupils midposition fixed irregular No caloric response flaccid or L.E. flexion Uncal herniation - early 3rd nerve Eupneic Dilate pupil, sluggish full or dysconjugate oculocalorics aversive movements, paratonia, Patient may be awake Uncal herniation Late 3rd nerve Sustained hyperventilation Dilated pupil, lid droops, Eye moves out and down Decorticate posturing Subtentorial lesions Pontine hemorrhage or infarction Tumors Cerebellar hemorrhage: if treated surgically before coma ensues, patient may achieve normal neurolgic recovery Signs point to one level and stay there Cranial nerve findings common Vertigo and nystagmus often prominent Initial diagnostic eval: all patients Lytes, BUN, Glucose Measured osmolality ABGs and cooximetry Urinalysis Selected studies for some patients Imaging LP Endocrine, Liver function Cultures (blood, CSF) Toxicology ECG Management Oxygen, ventilation, airway protection Circulation Glucose and thiamine, narcan lower intercranial pressure Control seizures Treat infection Correct acid-base disturbances Management Correct electrolytes Correct body temperature Specific antidotes Control agitation Oh yes, and our herniating lady Patient was intubated and hyperventilated Mannitol was given Neurosurgeon was paged stat He placed an intraventricular drain, clear CSF squirted across the room. . . And she woke up Patient was taken to angio suite where a 4 vessel revealed bilaterally greatly enlarged ventricles Dye down the drain revealed a noncommunicating hydrocephalus with block below the 4th ventricle Subsequent records from the warehouse revealed that she had been admitted for 6 months at age 18 months DX: Hydrocephalus residual from TB meningitis 18 yrs before Patient was given a Ventriculo-peritoneal shunt, was doing well 6 months later Lessons Her neck wasn’t stiff and she wasn’t resisting ROM, she had paratonia She had no focal findings because the lesions were bilateral and symmetrical Neurosurgeons are handy It’s better to be lucky than good Case 2 37 yo M found down at place of business at 5 am On arrival to ED: Tachypneic, tachycardic, hypertensive, diaphoretic and retching. Unresponsive to voice or pain. Pupils 2 mm bilaterally and unresponsive to light. Does not move extremities. Pt paralyzed, intubated and sedated What are the possible diagnoses? How should we work it up? Case 2 possible Diagnoses Mixed overdose with narcotic effect pupils possible but unlikely: narcan had no effect Intracerebral hemorrhage with intraventricular extension leading to sudden central herniation Primary pontine lesion, if onset were sudden, more likely a bleed than a stroke