Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
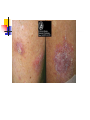
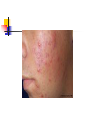
Primary Care Dermatology Dr Mick McKernan Description of skin lesions Papule Macule Nodule Patch Vesicle Bulla Plaque Papule Small palpable circumscribed lesion <0.5cm Macule Flat, circumscribed non-palpable lesion Pustule Yellowish white pus-filled lesion Nodule Large papule >0.5cm plaque Large flat topped elevated palpable lesion patch Large macule >2cm vesicle Small fluid filled blister < 1/2cm Bulla A large fluid filled blister > 1/2cm ECZEMA =dermatitis 10% of population at any one time 40% of population at some time Features of eczema Itchy Erythematous Dry Flaky Oedematous Crusted Vesicles lichenified Types of eczema Atopic Discoid eczema Hand eczema Seborrhoeic eczema Varicose eczema Contact and irritant eczema Lichen simplex Atopic eczema Endogenous Atopic i.e asthma, hay fever 5% of population 10-15% of all children affected at some time Atopic eczema individual must have: An itchy skin condition in the last 12 months+ three or more of: Onset before 2 years of age History of flexural involvement or flexural eczema currently present History of generally dry skin History of other atopic disease or FH Exacerbating factors Infection Teething Stress Cat and dog fur ? House dust mite ? Food allergens Clinical features Itchy erythematous patches Flexures of knees and elbows Neck Face in infants Exaggerated skin markings Lichenification Nail – pitted complications Bacterial infection Viral infections – warts, molluscum, eczema herpeticum ( refer stat). Keratoconjunctivitis Retarded growth Prognosis Most grow out of it 15% may come back – often very mildly Chronic skin dryness common after Treatment Avoid irritants especially soap Frequent emollients Topical steroids Sedating antihistamines – oral hydroxyzine Treat infections Bandages Second line agents Triple combination of therapy Topical steroid bd as required Emollient frequently Bath oil and soap substitute Principles of treatments Creams Ointments Amounts required Potential side effects Soap substitutes creams Cosmetically more acceptable Water based Contain preservatives Soap substitutes ointments Oil based Don’t contain preservative Feel greasy Good for hydrating Topical steroids Mild – “hydrocortisone Moderate – “eumovate” Potent – “betnovate” Very potent – “dermovate” Amounts required Emollients – 500g per week for total body FTU – steroids- the least potent that controls the symptoms. Bath oils – 2-3 capfuls per bath FTU Finger tip unit Helps to give estimation of topical steroid amount used To avoid over and under use of steroid FTU FTU 2 FTU = nearly 1 gram Enough for twice size of adult hand A hand and fingers (front and back) = 1FTU A foot (all over) + 2FTU Front of chest and abdomen = 7FTU Back and buttocks = 7FTU Face and neck = 2.5 FTU An entire arm and hand = 4 FTU An entire leg and foot = 8 FTU Discoid eczema Variant of eczema Easily confused with psoriasis Well demarcated scaly patches Limbs Often infective component (staph aureus) Hand eczema Pompholoyx – itchy vesicles or blisters of palm and along fingers Diffuse erythematous scaling and hyperkeratosis of palms Scaling and peeling at finger tips Hand eczema Not unusual in atopic More common in non atopics Cause often uncertain Irritants Chemicals Occupational history Consider patch testing – 10% positive Seborrhoeic eczema Over growth of yeast (pityrosporum ovale, hyphal form malassezia furfur) Strong cutaneous immune response More common in Parkinson’s and HIV Clinical features Infancy – cradle cap, widespread rash, child unbothered, little pruritus Young adults – erythematous scaling eyebrows, nasolabial folds, forehead scalp Elderly – more extensive Treatment Suppressive Mild steroid and antifungal combination Ketoconazole or dentinox shampoo Emollients Soap substitutes Venous eczema Gravitational = stasis eczema Lower legs Venous hypertension Inflammation Purpura pigmentation Clinical features Older women Past history DVT Haemosiderin deposition often misdiagnosed as cellulitis. Cellulitis is nearly always unilateral, tender and has a well demarcated edge treatment Emollients Topical moderately potent steroids Soap substitutes Compression – check arterial supply first Leg elevation Champagne bottle appearance of lipodermatosclerosis Lipodermatosclerosis and venous leg ulcer Cellulitis – unilateral painful and well demarcated. Asteatotic eczema =eczema craquele Dry skin Worse in winter Hypothyroidism Avoid soap Emollients Bath oils Contact and irritant eczema Exogenous Unusual Worse at workplace History of exacerbations irritant Can occur in any individual Repeated exposure to irritants Common in housewives, hairdressers, nurses –bleaches and chemicals contact Occurs after repeated exposure but only in susceptible individuals Allergic reaction Common culprits – nickel, chromates, latex etc Patch testing Lichen simplex =Neurodermatitis Cutaneous response to rubbing Thickened scaly hyperpigmentation Emotional stress May need biopsy to diagnose treatment Stop rubbing! Very potent steroids Occlusion PSORIASIS Psoriasis Affects 2% of population Well-demarcated red scaly plaques Skin inflamed and hyperproliferates Males and females equally Two peaks of onset (16- 22) and later (55-60) Usually family history Chronic plaque Extensor surfaces Sacral area Scalp Koebners phenomenon Guttate psoriasis Raindrop Children and young adults Associated with streptococcal sore throats Not all go onto get chronic plaque May resolve spontaneously over 1-2 months Guttate psoriasis Flexural psoriasis Later in life Well demarcated red glazed plaques Groin Natal cleft Sub mammary area No scale Treatment Step 1:Prescribe copious emollients - make the skin more comfortable and reduce the amount of scale Step 2:Dovobet is the most effective vitamin D analogue Avoid on areas of thin skin eg the face, flexures and the genitalia. Also consider dithranol and tar. Flares use topical steroids 2 weekserythroderma or generalised pustular psoriasis if overused. Step 3 : for hospitals. Phototherapy , cyclosporin , UV, methotrexate Step 4: biologicals : Etanercept, Infliximab, Adalimumab and Ustekinumab belong to the class of biological medicines called tumour necrosis factor (TNF) blockers. These work by blocking the activity of TNF. Erythrodermic and pustular psoriasis More severe > 90% involvement Need dermatologist! Usually need oral therapy Associated features Arthritis Nail changes- onycholysis, pitting, discolouration, subungal hyperkeratosis prognosis Chronic plaque tends to be lifelong Guttate – 2/3 further attacks, or develop chronic plaque ACNE VULGARIS Acne Vulgaris Common facial rash Usually adolescents 3% may persist after 25yrs especially women. Clinical features Increased seborrhoea Open comedones= blackheads Closed comedones= whiteheads Inflammatory papules Pustules Nodulocystic lesions scars Acne distribution Treatment Consider site Compliance Inflammatory/non inflammatory lesions Scarring Fertility Psychological effect Topical treatments Benzoylperoxidase – OTC, PanOxyl 5 to 10%, Azelaic acid – skinoren Antibiotics – clindamycin, erythromycin, steimycin Retinoids – adapalene Oral therapy Use if topical therapy ineffective or inappropriate Anticomedonal topical treatment may be required in addition Don’t combine topical with oral antibiotic as encourages resistance. 3 to 4 months before any improvement Antibiotics Oxytetracycline 500mg bd Tetracycline 500mg bd Doxycycline 100mg od Erythromycin 500mg bd Lymecycline 408mg od Hormone treatment for acne Dianette - not if COCP contraindicated Withdraw when acne controlled VTE occurs more frequently in women taking dianette than other COCP – caution ++ at this point. Oral retinoids Hospital only Long list of side effects Teratogenic Very effective Suicide- no proven link www.pcds.org.uk Rashes are difficult!