Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
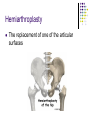
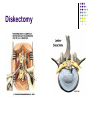
Nursing care of the Client with Musculoskeletal Stressors #2 Zelne Zamora, DNP, RN NRSG 308 Important Facts Age 65> = 90% of hip fx hosp. Females 2-3 times more likely Whites , Asians have higher incidence > 320,000 Americans hospitalized yearly More than 1.5 million osteoporotic fractures yearly Hip Fractures in the Elderly Risk Factors Age related BMD loss Chronic diseases Gender/Heredity Malabsorption Risk Factors Deficient nutrition Tobacco and alcohol use Medications Environmental hazards Hormone imbalances Public Enemy #1 OSTEOPOROSIS Reduction of bone density Change in bone structure Increase susceptibility to fracture Rate of bone resorption greater than bone formation OSTEOPOROSIS Loss of bone mass universal phenomenon associated with aging Calcitonin decreased Estrogen decreased PTH increased OSTEOPOROSIS Primary Occurs in women after menopause (usually 45-55 years of age) May occur in men later in life Failure to develop peak bone mass earlier in life due to lifestyle Secondary Result of medications, conditions, or diseases that affect bone metabolism Osteoporosis Genetics Gender Age Nutrition Physical exercise Lifestyle choices Medications Co-morbidity Osteoporsis – s/s Suboptimal nutrition of in children can contribute to disease Bones become progressively brittle and fragile Calcium Supplement Debate Children need RDA in the diet (recommended daily allowance) 12-15 y.o. modest benefit to spine 30-42 y.o. benefit with exercise only After menopause (45-55 y.o.) beneficial Osteoporsis – s/s Compression fractures common - pathological More common in women than men More common in Caucasians and Asians Osteoporosis Postmenopausal women Less tall – compression of spine curvature of spine, drooped posture Weak abdominal muscles – protruding abdomen Compression of lungs from posture – resp insufficiency The Available Evidence For Increasing Peak Bone Mass: RDA of CA+ and Vitamin D Exercise like an athlete 45 min at 80-90% maxHR 3 X wk Calorie intake adjusted to maintain energy balance Bone Mineral Density Testing Measures strength of bones Density of minerals, i.e., calcium Osteopenia – natural thinning of bones DEXA scan – way to measure BMD Bone Mineral Density Normal 2.5-1 below the young adult reference range (2.5 to -1) Osteopenia -1 to -2.5 Osteoporosis -2.5 or less Severe Osteoporosis -2.5 or less and presence of at least one bone fracture Drugs Used for Osteoporosis Estrogen Replacement Therapy Selective Estrogen Receptor Modulator Premarin Raloxifene (Evista) Calcitonin (Micalcin, Calcimar) Forteo (PTH) Biphosphonates Fosamax, Boniva, Zometa, Actonel Compression Fracture Hip Fracture Locations Signs and Symptoms Pain hip/groin Inability to put weight on injured leg Stiffness, bruising and swelling Shorter leg one side Leg turns inward or outward Screening and Diagnosis X-Rays Palpation Range of Motion Dexa Scan Hip fracture classifications Displaced Impacted Comminuted Displaced Impacted Comminuted Metal Screws Avascular Necrosis Death of tissue due to insufficient blood supply Broken bone interrupts blood supply Bone may collapse or reabsorb Avascular Necrosis Contributing factors Fractures Dislocations Slow intervention Prolonged corticosteroid therapy Treatment Traction may be ordered initially Metal screws Prosthetic Replacement Hemiarthroplasty Total hip arthroplasty (THA) Hip Replacement Hip Replacement Total Hip Replacement Replacement of the upper femur and the socket in the pelvic bone with a prosthesis Hip Replacement Total Hip Replacement Hemiarthroplasty The replacement of one of the articular surfaces Indications for THA Femoral neck fractures osteoporosis Osteoarthritis Rheumatoid arthritis Failure of previous prosthesis Avascular Necrosis Abductor pillow Activities to Avoid Avoid extremes of internal and external rotation, adduction, and 90 degree flexion of affected hip for 4-6 weeks post-op Use abduction pillow Avoid crossing the legs Use raised toilet seats Platform under chair Avoid twisting and reaching down, tying shoes, (use long- handled shoe horns and sock pullers) Prevention Strategies: Post-op Anti-embolism stockings – i.e., SCDs, TEDs Pneumatic compression devices Anti-coagulant therapy (LMWH or Coumadin) Fluid intake Prevention Strategies: Post-op Pressure ulcers Neuro-vascular - the 6 P’s Pain Paresthesias Pressure Paralysis Poikilothermia Pallor/Pulselessness Immobility A telectasis W asting of Bones F unctional loss of muscle U rinary Stasis L ast, but not least, constipation Postop complications DVT/ Fat Embolism/ PE Infection Pain Postop complications Urinary Retention Hip Dislocation Neuro-cognitive Delirium Depression Prevention of Hip Fractures Calcium & Vit.D Weight bearing No smoking/alcohol Treat osteoporosis HRT Home Safety Sensible shoes Eye exams Medication safety Total Knee Replacement Damaged bone and cartilage from your thighbone, shinbone and kneecap Replaced with an artificial joint (prosthesis) made of metal alloys, high-grade plastics and polymers http://www.edheads.org/activities/knee/ Total Knee Replacement Continuous Passive Motion Machine Continuous Passive Motion Machine Increases circulation and flexion to knee Usually patient is placed in CPM immediately after surgery Initially 0-40 degrees flexion to a goal of 090 degrees Increase 10 degrees every shift as patient tolerates Nursing Interventions Assess bleeding to dressing Reduce swelling CSM checks Peroneal nerve palsy Monitor drain output Know weight bearing status Complications DVT Peroneal nerve palsy Infection Limited range of motion Discharge Planning Musculoskeletal Complications Osteomyelitis Delayed Union Non Union Malunion Osteomyelitis Infection of the bone Can occur Through soft tissue infection Direct bone contamination Through bloodborne spread from other sites of infections Osteomyelitis Pathophysiology 70-80% of infection caused by Staphylococcus Areus Abscess formation occurs in the bone Scar tissue develops Low blood supply Leads to chronic osteomyelitis Signs and Symptoms Swelling Tenderness Warmth Constant pulsating pain May see drainage May see fever Treatment Remove drains ASAP Aseptic wound care Antibiotics Immobilization Hydration High protein diet Pain control Delayed Complications Delayed Union Nonunion Healing of the bone does not occur at normal rate Failure of the ends of the fractured bone to unite Malunion Failure of ends of fractured bone to unite in in normal alignment Treatment Internal fixation Bone grafts Bone healing stimulator Immobilization Non-weight bearing Educate on s/s of infection Cumulative Trauma Disorders (CTD’s) CTD’s: Work-Related Caused by repeated movements Can cause significant disability Are costly to society Carpal Tunnel Syndrome Treatment CTS Splinting Diuretics Vit B6 Treatment CTS Massage Ergonomic improvements Surgical decompression Low Back Pain 80% of Cases are Idiopathic Low Back Pain Prevention Reject sedentary lifestyle Build flexibility & strong abdominal muscles Use good body mechanics Proper positions Low Back Pain Prevention Ergonomics Stop smoking Maintain ideal weight Regular exercise Herniated Lumbar Disc Herniated disk Laminotomy Laminectomy Diskectomy Fusion Nursing Management Pain control PCA Respiratory care Incentive spirometer Cough and DB Nursing Management Proper positioning/ logrolling Neurovacsular checks (CMS) Turn q2 Look at activity orders Report deficit Monitor bladder and bowel function Nursing Management Mobility promotion Education No bending/twisting Fall prevention Use assistive devices as needed Assess home situation QUESTIONS