Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
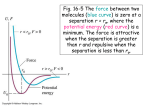
J005 1993 Syntex A ward Lecture Photomedicine and photodynamic therapy! DAVID DOLPHIN 2 Department of Chemistry, University of British Columbia, 2036 Main Mall, Vancouver; BC V6T 1Z1, Canada Received June 4, 1993 DAVID DOLPHIN. Can. J. Chern. 72,1005 (1994). Photodynamic therapy (PDT) involves the treatment of diseased tissue and cells using a photosensitizer and visible light. Such photomedical treatments have been known since the time of the ancient Egyptians but it was only just this year that this therapeutic modality was made available to modern medicine with the approval, in Canada, of Photofrin® for the treatment of bladder cancer. This paper reviews PDT with an emphasis on drug development, particulary for the second generation drugs. especially BPDMA (benzoporphyrin derivative-mono acid). which is now in human clinical trials. DAVID DOLPHIN. Can. J. Chern. 72,1005 (1994). La therapie photodynamique (TPD) implique Ie traitement des tissus et des cellules malades en utilisant un photosensibilisateur et la lumiere visible. De tels traitements photomedicaux sont connus depuis Ie temps des anciens Egyptiens, mais la medecine modeme n'a eu acces a cette modalite therapeutique que cette annee seulement avec I'approbation, au Canada, de la Photofine® pour Ie traitement du cancer de la vessie. Cet article revoit la TPD en mettant l' emphase sur la mise au point des medicaments, particulierement pour la deuxieme generation de medicaments et specialement la BPDMA (Ie derive mono-acide de la benzophorphyrine) qui est a I'essai c1inique chez les humains. [Traduit par la Redaction] Photo medicine has been practiced since at least the time of the ancient Egyptians (1). Psoralins from orally ingested plants accumulated in the skin and when activated by sunlight brought about repigmentation of the skin. This 4000-year-old treatment for vitilago is still used today with psoralins and UV exposure and represents the best known treatment even though it has only limited success. Indeed, a number of skin diseases, including acne, eczema, herpes simplex, and psoriasis, have been treated in a similar manner. Niels Finsen won the Nobel Prize in Medicine in 1903 for his treatment of cutaneous tuberculosis by UV radiation. However, the most promising areas of photomedicine are those that use a photosensitizer. Indeed, it was believed in the 19th century that all efficacious drugs were colored and while this belief led to the discovery of the sulfa drugs (Prontosil is an azo dye) it was not until the beginning of the 20th century that the medicinal properties of photosensitizers were explored. Raab (2) in 1900 showed that acridine dyes and light effectively killed Paramecia. In 1925 Policard (3) examined the ability of porphyrins, including hematoporphyrin (1), to produce a phototoxic effect. IThis Syntex Award Lecture was delivered by Professor Dolphin at the Annual Conference of the Canadian Society for Chemistry, Sherbrooke, Quebec, June 2, 1993. 2David Dolphin is the NSERC Industrial Research Chairholder in Photodynamic Technologies at the University of British Columbia and Vice President, Technology Development, at Quadra Logic Technologies Inc., Vancouver. Mayer-Betz injected himself with 200 mg of hematoporphyrin (4) and suffered no ill effects until he exposed himself to sunlight, whereupon he suffered extreme swelling and remained photosensitive for several months. Similar accumulation ofporphyrins in the skin of porphyric patients may cause severe skin necrosis upon exposure to strong light (5). Auler and Banzer in 1946 (6) showed that hematoporphyrin accumulated in cancerous tissues and, since it exhibits strong fluorescence, its localization into neoplastic and rapidly dividing tissue could be quantitatively assessed (7). Hematoporphyrin derivative HpD was first prepared by Schwartz and co-workers and its potential as a radiosensitizer was examined (8), but in 1964 Lipson et al. showed that HpD preferentially accumulated in cancerous tissue rather than in the surrounding healthy tissue (9-11). Interest in photomedicine and particulary photodynamic therapy (PDT) was rekindled when Dougherty (12) showed that HpD could be purified by gel exclusion chromatography, which removed monomeric porphyrins. The remaining oligomeric material is known as Photofrin® (2) and Quadra Logic Technologies, Vancouver (QLT), in partnership with Lederle Laboratories have just received a notice of Compliance from the Canadian Health Protection Branch for the use of Photofrin® in the treatment of superficial bladder cancer. Photodynamic therapy (PDT) requires that the photoactive agent first absorb a photon of a specific wavelength and in general the action spectra correlate well with the absorption spectra. As can be seen from the modified Yablonski diagram in Fig. 1, the first excited singlet state (SI) can fluoresce or this excited state can participate in an electron transfer process with a biological substrate, resulting in the photobleaching of the photosensitizer and modification (destruction/inactivation) of the substrate. This is known as a Type I photoprocess (13). PUVA (psoralin, 8-methoxypsoralin, plus UV radiation using UVA) relies on this photochemistry where the psoralin is believed to undergo photo addition to thymidine bases of DNA (14). In addition to being the most widely used treatment of psoriasis, PUVA also gives rise to cutaneous cancers (15). Photosynthesis using reduced porphyrins (chlorophylls, bacteriochlorophylls) makes use of a Type I process but the initially oxidized "porphyrin", at the reaction center, is reduced by another porphyrin 1006 CAN. 1. CHEM. VOL. 72,1994 R = HO-CH- or - I CH=CH2 and n = 0-7 CH3 PHOTOFRIN® (Profimer Sodium) (2) Sn _ __ S4 _ __ S3--S2 _ __ (1+) S, S, >- T, (tt) '-' 0::: W Z W Singlet 1 2 4 Triplet So , 2 3 - Absorption - Depends upon exti nction coefficient and wavelength Fluorescence - Lifetime depends on molecular interactions Intersystem crossing 4 5 - Phosphorescence , Conversion of triplet oxygen 3~ to singlet oxygen 02 FIG. 1. Modified Yablonski diagram. (cytochrome) such that no net destruction of the photoactive species occurs. A second, and far more interesting, photochemical process known as a Type II photoprocess results in the conversion of stable triplet oxygen 2 ) to the short-lived but highly reactive (toxic) singlet oxygen (102 ), This reaction occurs, as shown in Fig.!, when the S 1 state of the photosensitizer undergoes intersystem crossing to its first excited triplet state (T 1) followed by a triplet-triplet reaction with 302 to regenerate the photosensitizer in its ground state and singlet oxygen. Singlet oxygen has a lifetime of ~6 /Ls in water and a little longer in lipid and cell membranes, which means that it cannot diffuse more than a single cell length. Singlet oxygen is a powerful, fairly indiscriminant, oxidant that reacts with a variety of e0 biological molecules and assemblies. As shown in Fig. 2, oxygen atom transfer can result in the oxidation of both carbon and sulfur and in the formation of hydroperoxides from a variety of substrates including cholesterol and phosopholipids. The site of the greatest accumulation of the phototoxin may not define the site of cell death since, while a single oxidation of an amino acid in a protein may results in the shutdown of critical biological process (16--18), greater destruction ofless critical sites may be required for cell death. Be that as it may, Oleinick and colleagues (19) have shown that, in vitro, cells die by apoptosis 3 3 Apoptosis is programmed cell death involving endonucleosis and chromatin condensation. DOLPHIN ~H ~ 02 H NHl CH2-CH-COO- ~ lllstidine endoperoxides NH3+ NH3+ ~-CH-COO- ~-CH-COO- ~_OH H H Tryptophan hydroperoxide Tryptophan endoperoxide o NH3+ CH3-S-CH2-CH2-CH-COO- o o Methionine sulfoxide NHl HOS-CH2-CH-COO- Cysteine sulfenate NH3+ CH3-*-CH2-CH2-CH-cOO- II Methionine sulfone NHt H~S-CH2-CH-cOOCysteine sulfinate NHt HO;sS-CH2-CH-COO- Cysteine sulfonate FIG. 2. Typical examples of the reactions of singlet oxygen with biomolecules. after PDT. A dramatic example of cell membrane damage is shown in Fig. 3. This damage was observed (20) using BPDMA, which is discussed below. Since most photosensitizers currently in clinical trials for PDT (21) have quantum yields for singlet oxygen production of ~0.5 or higher, considerable amounts of singlet oxygen can be produced when the photosensitizer is illuminated with light of the appropriate wavelength. The penetration of light through tissue is attenuated by a number of factors but absorption and scattering are the most important in limiting the penetration depth for effective treatment. Heme proteins account for most of the absorption of light in the visible region. Since this drops off rapidly beyond 550 nm, the effective depth of penetration doubles in going from 550 to 630 nm (where Photofrin® is activated) and doubles again in going to 700 nm. However, beyond 700 nm only an additional 10% increase in penetration is achieved by moving into the infrared (Fig. 4). The clinical activation of Photofrin® at 630 nm was chosen since it has an absorption band there (albeit weak) that is stronger than the absorption of oxyhemoglobin at that wavelength (Fig. 5). Porphyrins (3) (Fig. 6) are 1871"-electron aromatic macrocycles that exhibit characteristics optical spectra with a very strong 71"-71"* transition around 400 nm (known as the Soret band) and four Q-bands in the visible region. As can be seen in Fig. 6, two of the peripheral double bonds, in opposite pyrrolic rings, are crossed conjugated and are not required to maintain 1007 aromaticity. Thus reduction of one or both of these cross-conjugated double bonds (to give chlorins (4) and bacteriochlorins (5) maintains aromaticity but the change in symmetry results in bathochemically shifted Q-bands with high extinction coefficients (Fig. 6). Nature uses these optical properties of the reduced porphyrins to harvest solar energy via photosynthesis with chlorophylls and bacteriochlorophylls as both antennae and reaction center pigments. The long-wavelength absorptions of these chromophores naturally led to explorations of their use as phototoxins in PDT where they have exhibited some interesting properties (22, 23). Nevertheless, the complexity of these natural pigments and the considerable problems in their isolation, separation, and purification add to the difficulties in their development for clinical use. Moreover, chlorins and bacteriochlorins, by virtue of their di- and tetrahydro reduction states, can be readily oxidized back to the parent porphyrin accompanied by the loss of their long-wavelength absorption bands. This potential lack of stability has led us to examine other ways of producing stable chlorin-like chromophores. Protoporphyrin IX as its iron complex (heme) is the prosthetic group of heme proteins and is thus readily available from a number of animal sources. As a result of the cross-conjugated nature of the peripheral double bonds it seemed likely that one of these double bonds and a conjugated vinyl group of protoporphyrin IX might act as a diene in a Diels-Alder reaction (24). When protoporphyrin IX dimethyl ester (6) is treated with a strong dienophile such as tetracyanoethylene, both 2 + 2 and 2 + 4 cycloadditions take place on either or both rings A and B (Scheme 1) (24). Acetylene dicarboxylic ester, on the other hand, brings about a Diels-Alder reaction at either ring A or B but we have not seen reaction at both rings (25). The initially formed cycloadducts (7,8) are 1,4-cyclohexadienes having strong absorptions at 666 nm consistent with their chlorin-like chromophores (Fig. 7). Treatment of the 1,4-diene with triethylamine tautomerizes it to the 1,3-diene (9). This conjugated chlorin absorbs at 686 nm and turns out to be a kinetically controlled product having a cis arrangement of the angular methyl and methoxycarbonyl groups. Treatment of this cis-l ,3-diene or the original l,4-dienes with 1,5-diazobicyclo[5.4.0lundec-5ene (DBU) generates the thermodynamically more stable trans product (11). X-ray crystallography confirms the structure and stereochemical assignments made from previous NMR studies (Fig 8) (26). The cis and trans isomers both exhibit strong absorption around ~690 nm (Fig. 7). Prolonged treatment of the 1,3-dienes with TEA eliminates the angular methyl group and generates the benzoporphyrin (10), which has a characteristic porphyrin spectrum (Fig. 7). Hydrolysis of the dimethyl ester in concentrated HClleaves the ester groups on the exocyclic ring intact owing to steric hindrance experienced by the group close to the angular methyl and the conjugation of the other. The propionic esters do hydrolyze to give a mixture of the diacid (14) and the two regioisomeric monacid monoesters (12, 13). Cytotoxicity studies using the diacid showed that it was 10-70 times more cytotoxic than hematoporphyrin against a variety of normal and malignant cell lines (27). Surprisingly, a comparison of the photo toxicity of the monoacids showed that they were five times more cytotoxic than the corresponding diacids (28) for both the ring A and ring B analogs (Fig. 9). We choose to proceed towards clinical trials using the two regioisomeric monoacids of the ring A analog (12 and 13) that we call BPDMA (benzoporphyrin derivative ring o o 00 n » z ~ n ::r: tTl s: o< r- -.J J" -0 -0 """ FIG. 3. Feline T cells were treated with 2 j.Lg/mL of BPDMA and light. A: uninfected cells and light show no damage; B. infected (with FeIV) cells after early treatment with light show small holes in the membrane, as light treatment continues, the holes increase in size (C) until the membrane eventually appears to be completely destroyed (D). Reprinted by permission form Blood Cells (20). 1009 DOLPHIN .c +' 100% Q. Q) '0 .... 10 I :::g C 0 :;; (1j ,, ,,",, l- +' Q) f \ C ,, ,, Q) Q. .' Q) :' > :;; (,) Q) 300 :t: Q) 500 700 900 1100 Wavelength (nrn) Q) > FIG. 5. Optical spectra of oxyhemoglobin (--) and Photofrin® +' (----). (1j Q) 0: 550 630 800 700 nm FIG. 4. Relative depth of penetration, in muscle, of light of various wavelengths. A mono acid), whose optical spectrum (Fig. 10) shows a maximum absorption at the wavelength (~690 nm) where blood has a minimum absorption. While BPDMA does not show specific affinity for tumors, it exhibits significantly higher concentrations in tumors than in the surrounding healthy tissues (29). BPDMA localized in tumors better than in other tissues except liver, kidney, and 300 400 500 600 WAVEl..£NGTH (nm) 700 400 spleen. BPDMA is a chemically stable powerful phototoxin (its quantum yield for singlet oxygen is 0.46 (30)); however, before proceeding with the extremely expensive and time- consuming preclinical studies needed before a health board will issue an IND (investigation of a new drug), which allows the undertaking of human clinical trials, one is well advised to examine the extent of prolonged skin photosensitivity. Photofrin® causes skin photosensitivity in patients for 4-6 weeks after treatment. This is a minor side effect compared to those experienced with chemotherapy or radiation therapy; nevertheless, a successful second generation phototoxin for PDT must exhibit dramatically reduced skin photosensitivity compared to Photofrin®. As can be seen from Fig. 11, compounds 12, 13, and 14 all showed rapidly decreasing skin photo- 500 600 700 WAIJEl.ENGTH (nm) 500 600 700 WAVElENGTH (nm) Porphyrin Chlorin B acteriochlorin 3 4 5 BOO FIG. 6. Structures of the porphyrin (3), chlorin (4), and bacteriochlorin (5) macrocycles. The cross-conjugated double bonds in 3 can be reduced, leaving the dihydro (4) and tetrahydro (5) analogs aromatic. Increasing reductions result in an increasing bathochromic shift of the lowest energy absorption band. 1010 CAN. J. CHEM. VOL. 72,1994 NC CN ~ ~~ NH NC CN NC CN 'C=C"'" ..... , "- .... CN CN CN ;.r N~NCCNCN NC 6 NC I NC N NC,,- Me02CC=CC02Me Me02C B'<II. N- NC CN CN NC C02Me C02Me 1 ~ ....., ~ N- ;.r C02Me TEA 7 ~ 8 9 DBU SCHEME 1 BPDMA is virtually insoluble in water and it has been formulated in unilamellar liposomes to make it water soluble. There is evidence to suggest that tumor selectivity with hydrophobic photosensitizers may be mediated by plasma proteins, especially low-density lipoproteins (LDL) (31-33). BPDMA associates predominantly with LDL (34) and, when preassociated with LDL improved delivery to tumors in a mouse tumor model was seen (35). The unilamellar liposomes rapidly deliver the BPDMA to the lipoprotein fraction when placed in serum, and PDT in a mouse tumor model showed that the liposomally formulated material accumulated more rapidly when delivered in this fashion than when injected in DMSOIPBS (36). 300 400 500 600 WAVELENGTH (nm) 700 FIG. 7. Optical spectra of the 1,4-diene (7,··· .), the 1,3-diene (11, --), and the benzoporphyrin (10, - - - -). sensitivity compared to Photofrin®, and after 72 skin photosensitivity had almost returned to normal with the monoacids. At this stage we were anxious to see if this minimal skin photosensitivity would also be seen with humans. As long as a phototoxin preferentially accumulates in diseased tissue, or in a pathogen, then differential damage occurs when the system is illuminated. Under such conditions an appropriate drug dose - light energy combination can be found whereby the diseased tissue or pathogen can be destroyed without causing irreversible damage to healthy tissues. Photobleaching (37), a type I photoprocess that occurs more readily in vivo than in pure organic or aqueous solvents, may assist in minimizing damage to healthy tissue if photobleaching of low concentrations of the phototoxin in healthy tissue is complete 1011 DOLPHIN FIG. 8. X-ray structure of a BPD derivative drawn by Biosym's InsightII. 100 ..... -0 IS (]) 0 80 ...I ~ (fJ :::2l 60 (]) ""b...... U ~ 10 40 I I 5 ~ ,\ tV '..1I " , J :x2 20 10 100 1000 Concentration (ng/mL) FIG. 9. In vitro cytotoxicity BPDMA (12 and 13, .), the corresponding monoacid monoester derivatives of the ring B analog ( ), the diacid (14, e), and the analogous ring B diacid (D) examined under the same conditions (28). before irreversible damage can take place. Photofrin® and BPDMA photobleach at similar rates. 4 While we are just beginning to understand the mechanisms by which phototoxins biodistribute, few structure-activity relationships are known. Nevertheless, BPDMA has a great propensity to accumulate in diseased cells and in the neovasculature of hypoproliferic tissues. Measurements of biodistribution are aided by the strong fluorescence at 690 nm shown by BPDMA (Fig. 12). Fluorescence-activated cell-sorting (FACS) analysis following excitation in the UV at 420 nm showed dramatic differences between several leukemic cell lines, leukemic clinical isolates, and normal bone marrow cells incubated with BPDMA (38). Indeed BPDMA shows great potential for the ex-vivo purging of residual tumor cells in autologous bone marrow grafts. A four-log elimination of tumor cells occurred after a l-h incubation with 75 ng/mL BPDMA followed by exposure to white light; at the same time pluripotent stems, the progenitors for all hemopoietic cells, survived the purging regime (39). Human clinical trial using BPDMA to purge leukemic autolysis grafts wiII begin this year under the direction of QLT. Numerous viruses, pathogenic to humans, contain an outer hydrophobic membrane (envelope). Included amongst these viruses are cytomegatovirus (CMV), herpes simplex virus 4W.R. Potter. Personal communication. Wavelength (nm) FlO. 10. Optical spectra of oxyhemoglobin (--) and BPDMA (- -). .i!:" 6 ';;;: :;:: 'iii c: 5 ~ 4 Q. 3 CD +- o ..c: 1m BPD-MA iii BPD-MB ml BPD-DA D Photofrin® c: ::;: II! 2 CD > :;:: a G.i O! o 48 72 24 3 Time post injection (h) FlO. 11. Skin photosensitivity in mice following Lv. injection of the photosensitizers (4 mglkg) and exposure to white light (95 J/cm\ Severe damage resulting in eschar formation was scored as 5 (47). Compounds are described in Fig. 9. (HSV), several of the hepatitis viruses, and retroviruses such as the human T cell leukemic virus (HTLV) and human immunodeficiency virus (HIV). These, and other viruses, may be transmitted in transfused blood but it has been shown, using 1012 CAN. 1. CHEM. VOL. 72,1994 100 t..J , t) ,1, I Z t..J ,I'I t) (/) t..J c:::: 50 => I I' I I I I I ' 1 I I I I • , I 1 I I 0 ....J I..&... I II I . • I \ I " ... _-..... O~TTTlnn,.TTrrMnIlTTrrM 300 400 500 600 700 WAVELENGTH (nm) 800 FIG. 12. Fluorescence (- - - -) excitation (--) spectrum of BPDMA -:::J 1,000 E 500 " 0> C '-' Z <0 200 100 ::::el(/)< 50 o..Z 20 ~g: l.LI () z 0 () 10 5 a 6 12 18 24 TIME (h) FIG. 13. Plasma concentrations of BPDMA in patients following an i. v. infusion of the drug at 2.5 mg/kg. vesicular stomatitis virus (VSV) and feline leukemia virus (FeLV) as models, that BPDMA and light were effective in eliminating both cell-free virus and virally infected cells while at the same time leaving the red cells apparently undamaged (20, 40). Further studies have shown that BPDMA is effective for the elimination of both free and virally infected leukocytes in whole blood from virally infected humans under conditions that appeared to spare both the red cells and uninfected leukocytes (41). On the basis of these results and other preclinical studies, QLT plan to initiate clinical trials for the extracorporeal treatment of HIV -infected patients. The benefits of reducing the viral load must await the results of the clinical trials. In addition to reducing the viremia, other immunologic effects may be found as were observed after PDT with Photofrin®. Immunosuppression, as indicated by sensitivity to dinitrofluorobenzene (42), was observed in mice after PDT and an increase in chronic inflammatory cells was observed in patients after treatment for bladder cancer using Photofrin®. Moreover, the release of cytokines such as interleukin-l band -2 and the release of tumor necrosis factor by macrophages (43,44) and of thromoxane (45) have all been observed shortly after PDT. While several second generation drugs are in clinical trials (21), the most advanced and most promising is BPDMA, which is being used on a number of cutaneous cancers including basal cell carcinoma, metastatic breast and gastrointestinal carcinomas, and metastatic amelanotic melanoma as well as for the treatment of psoriasis. At the present time the drug is infused in doses ranging from 1.5 to 5.0 mg/kg and light doses, administered 3 h later, have ranged from 25 to 150 J/cm 2 • More than 70 cutaneous tumors have been treated and followed for several months after treatment. Complete responses were observed for the higher drug and light doses, and overall tumor responses of greater than 60% has been recorded (46). These exciting and promising results are being paralleled in the treatment of psoriasis where only a few patients have so far been treated. We noted above that any successful second generation photosensitizer must exhibit minimally prolonged skin photosensitivity if it is to be successful in the clinic. The pharmacokinetic profile for BPDMA in human serum concentrations is shown in Fig. 13 where rapid clearance from the system is clearly observed. This decrease in serum levels is paralleled by a lowering of skin photosensitivity with time. A major purpose of the first phase of the clinical trial was a measurement of skin photosensitivity, and extensive studies using UVA and visible light from a solar simulator (using a filtered xenon arc lamp) have been carried out (46). Marked skin photosensitivity was observed shortly after treatment but photosensitivity shows a logarithmic decrease with time and it is expected that skin photosensitivity will return to normal (pre-BPDMA infusion) within 1-2 days at the expected clinical dose of BPDMA. BPDMA thus seems to be meeting all of the necessary and hoped-for requirements of a successful second generation photosensitizing drug and, as the only non-mutagenic, non-carcinogenic, non-(dark) toxic anti-cancer drug known, we anticipate its use in a variety of clinical situations. Acknowledgements This work was supported by the Natural Sciences and Engineering Research Council of Canada (NSERC) and Quadra Logic Technologies Inc. L 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. M.F. Edelson. Sci. Am. 259, 68 (1988). O. Raab. Z. BioI. 19, 524 (1900). A. Policard. c.R. Hebd. Soc. BioI. 91, 1422 (1924). The physiological effects of radiation energy. Edited by H. Laurens. Tudor Press, New York. 1933. L. Eales. In The porphyrins. VoL VI. Edited by D. Dolphin. Academic Press Inc., New York. 1979. p. 663. H. Auler and G. Banzer. Z. Krebsforsch. 53, 65 (1942). F.H.1. Ftigge, G.S. Wieland, and L.O']. Mungariello. Proc. Soc. Exp. BioI. Med. 68, 640 (1948), TJ. Dougherty, B.W Henderson, S. Schwartz, lW Winkelman, and R.L. Lipson. In Photodynamic therapy. Edited by RW Henderson and TJ. Dougherty. Marcel Dekker Inc., New York. 1992. p. L R.L. Lipson, EJ. Blader, and E.M. Olsen. J. NatL Cancer Inst. 26, 1 (1961). R.L. Lipson, M.J. Gray, and EJ. Blades. Proc. IX lnt. Cancer Congr. 9th, Tokyo. 1966. p. 393. TJ. Dougherty. Cancer Res. 38, 2628 (1988). T.1. Dougherty. Photochem. PhotobioL 46, 569 (1987). EJ. Kapinus, M.M. Weksankia, V.P. Starzi, V.I. Boghillo, and LL Dilung. J. Chern. Soc. Faraday Trans. 2, 81, 631 (1985). J.A Parrish, TR Fitzpatrick, L Tanenbaum, and M.A. Puthak. N. EngL J. Med. 291, 1207 (1974). 1.H. Epstein. 111 The sciences of photobiology. Edited by K.C. Smith. Plenum Press, New York. 1989. p. 155. DOLPHIN 16. E. Ben-Hur, A. Orenstein, A. Livinc, and I. Rosenthal. Laser Life Sci. 3, 255 (1990). 17. K.1.A. Davies, S.W Lin, and R.E. Pacitici. J. BioI. Chern. 262, 9914 (1987). 18. C. Prinsze, T.M.A.R. Dubbelman, and J. Van Steveninck. Biochim. Biophys. Acta, 1038, 152 (1990). 19. M.L. Agarwal, M.E. Clay, E.J. Harvey, H.H. Evans, and N.L. Oleinick. Cancer. Res. 51, 5993 (1991). 20. J. North, H. Neyndorff, D. King, and J.G. Levy. Blood Cells, 18, 129 (1992). 21. E.D. Sternberg and D. Dolphin. J. Clin. Laser Med. Surgery. In press. 22. R.P. Allen, D. Kessel, R.S. Tharratt, and N. Volz. In Photodynamic therapy and biomedical lasers. Edited by P. Spinelli, M. Dal Fante, and R. Marchesini. Elsevier Science Publishers B.Y., The Netherlands. 1992. p. 441. 23. K.M. Smith, S.-J. Lee, F.-Y. Shian, R.K. Pandey, and N. Jagerovic. In Photodynamic therapy and biomedical lasers. Edited by P. Spinelli, M. Dal Fante, and R. Marchesini. Elsevier Science Publishers B.Y., The Netherlands. 1992. p. 769. 24. Y. Scherrer Pangka, A.R. Morgan, and D. Dolphin. J. Org. Chern. 51, 1094 (1986). 25. R.K. DiNello and D. Dolphin. J. Org. Chern. 45, 5196 (1980). 26. E.D. Sternberg, S. Rettig, and D. Dolphin. Manuscript in preparation. 27. A.M. Richter, B. Kelly, J. Chow, D.1. Liu, G.H.N. Towers, D. Dolphin, and J.G. Levy. J. Natl. CancerInst. 79, 1327 (1987). 28. A.M. Richter, E. Waterfield, A.K. Jain, E.D. Sternberg, D. Dolphin, and J.G. Levy. Photochem. Photobiol. 52, 495 (1990). 29. A.M. Richter, S. Cerruti-Sola, E.D. Sternberg, D. Dolphin, and J.G. Levy. J. Photochem. Photobiol. B: 5, 231 (1990). 30. E.D. Sternberg, D. Dolphin, R. Scurlock, M. Rougee, and R. Bensasson. Photochem. Photobiol. In press. 31. G. Jori, E. Beltramini, E. Reddi, B. Salvato, A. Pagnan, L. Ziron, L. Tomio, and T. Tsanov. Cancer Lett. 24, 291 (1984). 1013 32. D. Kessel. Cancer Lett. 33, 183 (1986). 33. P. Morliere, E. Kohen, J.P. Reyftmann, R. Santus, et. al. Photochern. Photobiol. 46, 183 (1987). 34. B. Allison, P.H. Pritchard, Richter, A.M., and J.G. Levy. Photochern, Photobiol. 46, 501 (1990). 35. B. Allison, E. Waterfield, A.M. Richter, and J.G. Levy. Photochern. Photobiol. 54, 709 (1991). 36. A.M. Richter, E. Waterfield, A.K. Jain, A.1. Canaan, B.A. Allison, and J.G. Levy. In Photodynamic therapy and biomedical lasers. Edited by P. Spinelli, M. Dal Fante, and R. Marchesini. Elsevier Science Publishers B.Y., The Netherlands. 1992. p. 549. 37. L.O. Svaasand and W.R. Potter. In Photodynamic therapy. Edited by B.W. Henderson and T.1. Dougherty. Marcel Dekker Inc., New York. p. 369. 38. C.H.M. Jamieson, WN. McDonald, and J.G. Levy. Leuk. Res. 14, 209 (1990). 39. R.M. Lemoli, T. Igarashi, M. Knizewski, L. Acabu, A. Richter, A. Jain, D. Mitchell, J. Levy, and S.c. Galati. Blood, 81, 793 (1993). 40. J. North, S. Freeman, J. Overbaugh, J. Levy, and R. Lansman. Transfusion, 32, 121 (1992). 41. J. North, R. Coombs, and J. Levy. In Photodynamic therapy and biomedical lasers. Edited by P. Spinelli, M. Dal Fante, and R. Marchesini. Elsevier Science Publishers B.Y., The Netherlands. 1992. p. 103. 42. C.A. Elmets and K.D. Brown. Cancer Res. 46, 1608 (1986). 43. S. Evans, W. Matthews, R. Perry, D. Fraker, J. Norton, and H.I. Pass. J. Natl. Cancer Inst. 82, 34 (1990). 44. D.A. Bellnier. Photochem. Photobiol. 8, 203 (1991). 45. Y.H. Fingar, T.1. Wieman, and K.W Dunk. Cancer Res. 50, 2599 (1990). 46. H. Lui, L. Hruza, N. Kollias, J. Wimberly, V. Salvatori, and R.R. Anderson. Proc. SPIE-Int. Soc. Opt. Eng. 1876, 147 (1993). 47. A.M. Richter, S. Yip, E. Waterfield, P.M. Logan, C.E. Stonecker, and J.G. Levy. Photochem. Photobiol. 53, 281 (1991).