Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
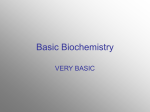
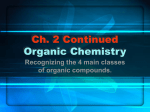
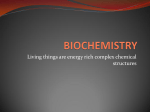
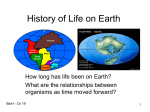
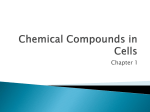
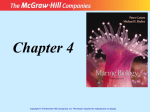
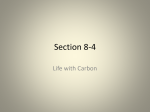
1909 Journal of Applied Sciences Research, 9(3): 1909-1916, 2013 ISSN 1819-544X This is a refereed journal and all articles are professionally screened and reviewed ORIGINAL ARTICLES Detection of Urinary Organic Acids in high risk Egyptian Children by Electrospray Tandem Mass Spectrometry 1 El-Mesallamy H., 2Gouda A., 2Fateen E., 2Elbaz A 1 Biochemistry Department, Faculty of Pharmacy, Ain Shams University, and Department, National Research Centre, Giza, Egypt. 2 Biochemical Genetics ABSTRACT Establishing an approach for early diagnosis and monitoring of disorders associated with accumulation organic acids in high risk Egyptian children using liquid chromatography tandem mass spectrometry (LC/MS/MS). Organic acids were detected in urine using LC/MS/MS and results were then confirmed by gas chromatography/ mass spectrometry (GC/MS). For confirmation of the type of organic acidurias (OA), acylcarnitines and/ or amino acids profiles using LC/MS/MS were done to all patients showing abnormal organic acids profiles patterns. LC/MS/MS detection of urinary organic acids revealed 31 out of 50 subjects (62%) with 11 different OAs. Organic acids profile must be done to neonates admitted to critical care units suffering unexplained neurological manifestations. The LC/MS/MS is a fast and efficient technique for the detection of many organic acids in urine and can facilitate the future screening for OA among high risk Egyptian families. Key words: Electrospray tandem mass spectrometry, organic acidurias, inborn errors of metabolism, toxic encephalopathy, neonatal screening. Introduction Organic acidurias(OA) are diverse group of inheritable genetic metabolic disorders characterized by accumulation of non-amino organic acids in urine; these disorders share the characteristic of having neurological manifestations as the main clinical presentation. Although the individual incidence of each type of OA is very low, the cumulative incidence of OA as a group is high. (Hoffmann, 1994). Due to high consanguinity in Egypt, OA, like most other inborn errors of metabolism (IEM), are found in many families and cause high morbidity and mortality rates due to neurological damages which happen at a very young age. These disorders are mostly misdiagnosed as other non-inheritable disorders such as sepsis, neonatal asphyxia, or poor feeding, leading to wasting a lot of time that is very precious to the patients because the neurological damages are usually irreversible. (Kamboj, 2008; Fateen et al., 2009). All over the world, screening neonates just after their birth allows the early detection of some types of IEM; hence, affected neonates are diagnosed before they develop their 1st symptoms. (Dionisi-Vici et al., 2006). The diagnosis of OA is very difficult and needs a very careful and accurate interpretation of both the clinical presentation and the biochemical parameters of the patient. The diagnosis depends mainly on clinical presentation as well as detection of urinary organic acids using gas chromatography coupled to mass spectrometry (GC/MS). (Sweetman, 1999). The aim of this study is to establish an approach for early diagnosis and monitoring of disorders associated with accumulation organic acids in high risk Egyptian children using LC/ MS/ MS. In order to ensure that the results obtained by LC/ MS/ MS are correct, the same samples were analyzed using GC/MS. Confirmation of the type of OA for each patient is carried out using assay of amino acids as well as acylcarnitines profiles in dried blood spots. Materials and Methods Organic acids profile was carried out for all patients and controls using LC/ MS/ MS according to the method of Pitt et al., (2002). In this method a 200μL of a solution containing 5μmol/L Hexanoyl [13C2] glycine (internal standard) in acetonitrile: H2O (1:1 by volume) was added to the urine samples with volumes equivalent to a creatinine concentration of 20nmol/L and injected directly using Finnigan Surveyor autosampler into HPLC-ESI-MS system consisted of an HP 1100 Series HPLC instrument(quaternary pump and degasser, Corresponding Author: Dr. AmrSobhi Gouda, Assistant professor of biochemical genetics department. National research center, El-Bohouth Street, Dokki, Giza, Egypt. E-mail: amr_gouda3@yahoo.com, ph: +201001440865 1910 J. Appl. Sci. Res., 9(3): 1909-1916, 2013 column compartment, and autosampler)and an LCQ ADVANTAGE MAX mass spectrometer from Thermo Finnigan. Nitrogen was used as a sheath gas. Helium was used as collision gas at a pressure of 2.5 to 3.5mTorr. The collision energy was set to 35eV. Temperature was set to70oC. Data were collected and analyzed using Xcaliber 1.4 software. Each organic acid was identified on basis of its mass to charge ratio (m/z) and confirmed by the m/z of its daughter ion. Another urine sample for the same patient or control was analyzed for its organic acids content using GC/ MS according to the method of Sweetman (1991). In this method a urine sample with volume equivalent to a creatinine concentration of 1mmol/L was made up to 2mL with distilled water acidified to pH 1.5 and mixed with 100μL of decanoic acid 5mM/L and 100μLof heptadecanoic acid 75mg/ 200mL (internal standards). Solid sodium chloride was added and the organic acids were extracted twice with 2mL ethylacetate then once using diethyl ether. The organic acids were pooled and evaporated under nitrogen. Drevatization was then performed with 75μL of BSTFA (bis-trimethylsyliltrifluracetamide + 1% trimethylchlorosilane) and 20μL of pyridine in a fume cupboard to each dried extract, the extract was heated for 30 minutes at 80oC and then transferred into GC/MS vials. A half μL of the drevatized sample was injected into GC/MS instrument with a CP-sil 8 CB capillary column. The temperature settings were as follows: Injector 250oC, column 90- 280oC with an increment of 3oC per min, ion source 150oC and mass analyzer 35oC. Organic acids were analyzed based on both retention time (Rt) and fragmentation pattern. According to the type of OA, acylcarnitines, and/ or amino acids profiles in dried blood spot using LC/ MS/ MS according to the methods of Schulze et al (2003) and Zoppa et al (2006) were done respectively. Subjects having normal organic acids profile but experienced intermittent attacks of neurological signs and symptoms with symptoms free intervals were asked to repeat the tests using samples taken during the episodes to ensure that organic acids profile is normal in presence and absence of signs and symptoms. Patients: The study included 50high risk Egyptian children referred to the biochemical genetics department from different university hospitals, ICU and private clinics. The selection criteria: - Patients with a +ve family history of OA and had unexplained neurological manifestations. - Patients with -ve family history of OA but had unexplained neurological manifestations. - Normally apparent neonate having brothers or sisters previously diagnosed as patients of OA. Patient ages ranged from 1month to 51 months. Twenty healthy controls of matching ages were also included for comparison. A written consent was signed by the parents or care takers of the studied subjects and controls after full explanation of the study. This consent was obtained from the ethical committee at the National Research center (NRC). All patients and controls were subjected to full history taking and physical examination. Results: The present study included 50 patients. The study included 27 boys (54 %) and 23 girls (46 %). Thirty three (66 %) from the studied cases were born to consanguineous parents. Detection of urinary organic acids revealed 31 cases with 11 different types of OA. These OAs and their accumulated organic acids are shown in table (1). Discussion: Many studies have shown that OAs are relatively common disorders among the IEM (Hori et al, 2005; Keeratichameron et al., 2005; Wasant et al., 2008; Wagner et al., 2009). The diagnosis of OA depends on clinical presentation as well as the detection of organic acids in urine. Isovaleric acidemia (IVA) was the first detected OA by Tanaka using GC/MS in 1966. (Tanaka et al., 1966). The present study was constructed to establish a diagnostic approach for early diagnosis of various disorders associated with accumulation of organic acids in urine of high risk Egyptian children. The highest presentation of our study group was in the 2nd year of life. Taking the history of the patients, the delayed diagnosis was attributed to the lack of awareness of the physicians about the signs and the symptoms of a genetic disorder and how to differentiate it from other non-inheritable disorders and, as a result, patients remained completely undiagnosed or were misdiagnosed with non-inheritable disorders and were subjected to recurrent metabolic crises with its concomitant irreversible damage. That was obvious in three of our patients who died affected by the complications of their diseases shortly after presentation. These patients were diagnosed either with tyrosinemia or multiple acyl CoA dehydrogenase deficiency (MADD). 1911 J. Appl. Sci. Res., 9(3): 1909-1916, 2013 Table 1: Types of OA detected in this study with the abnormal metabolites detected by LC/ MS/ MS. Percent Percent Number of from from Acylcarnitines OA patients total diagnosed Organic acids profile profile diagnosed number cases (n=50) (n=31) MSUD 6 Multiple carboxylase deficiency PKU GA I 12% 19.4% 4 8% 12.9% 4 8% 12.9% 4 8% 12.9% Orotic aciduria 3 6% 9.7% MMA 3 6% 9.7% MCADD 2 4% 6.5% Tyrosinemia I 2 4% 6.5% MVA MGA 1 1 2% 2% 3.2% 3.2% MADD 1 2% 3.2% 2-oxoisocaproate & 2hydroxyisovalerate Lactate, 3-hydroxypropionate, 3hydroxyisovalerate and C5:1 glycine. Phenyllactate, phenylpyruvate and phenylacetate C5dicarboxylate and 3hydroxyglutarate Orotic acid Lactate, methylmalonate, 3hydroxypropionate and methylcitrate C6- 10dicarboxylic acids, suberyl glycine and hexanoyl glycine. 4-hydoxyphenylpyruvate, 4hydoxyphenyllactate, 4hydroxyphenylacetate and succinylacetone. Mevalonate and mevalonolactone Methylglutaconate Lactate, C4dicarboxylate C5dicarboxylate and Amino profile Leucine valine - acids and Alanine - Phenylalanine C5 DC acylcarnitine - - None in 1 patient and citrulline in 2 patients with orotic aciduria. C3acylcarnitine Alanine glycine C6-C10 acylcarnitines - - Tyrosine C4, C5, C6, C8, C10, C12, C14, C16 and C18 Leucine valine and and (-) Non significant Figures (1-4) show a case with MMA diagnosed through organic acids profile followed by acylcarnitines and amino acids profiles. Subject#17 #5-307 RT: 0.08-2.99 T: - cESI Full ms [ 50.00-320.00] 3-OH Propionate and Lactate 140000 89.25 C4 Dicarboxylate 130000 Internal standard 120000 117.25 110000 174.21 100000 Methylcitrate Intensity 90000 80000 70000 205.02 60000 50000 40000 144.11 30000 20000 10000 91.64 81.62 107.59 234.91 166.36 179.73 265.41 287.45 257.23 0 50 100 150 200 250 300 m/z Fig. 1: Negative ion spectrum for patient with MMA using LC/ MS/ MS. The organic acids profile shows peaks of Lactate & 3-Hydroxypropionate (m/z=89), C4 Dicarboxylate (m/z=117) and Methylcitrate (m/z=205). 1912 J. Appl. Sci. Res., 9(3): 1909-1916, 2013 2000000 Methylmalonate 1900000 Lactate 1800000 Methylcitrate 1700000 1600000 1500000 1400000 1300000 Internal standard 1200000 Abundance 1100000 1000000 900000 800000 700000 600000 Internal standard 500000 400000 300000 200000 100000 0 0.0 4 8 12 16 20 Time (min) 24 28 32 36 Fig. 2: Chromatogram for a case with MMA using GC/ MS. Organic acids profile shows peaks of Lactate, Methylmalonate and Mehylcitrate. Subject#17 RT:0.73 T: + cESI Full ms [200.00-500.00] 100 C3 95 274 90 85 80 75 70 Intensity % 65 60 55 50 45 304 40 35 30 25 * 263 15 10 d3C3 459 20 227 218 260 347 277 456 5 0 250 300 350 m/z 400 450 500 Fig. 3: Acylcarnitines profile for a case with MMA showing the characteristic peak for C3 acylcarnitine. 1913 J. Appl. Sci. Res., 9(3): 1909-1916, 2013 Subject #17 RT: 0.84 T: + cESI Full ms [ 50.00-300.00] 90 100 Alanine 95 90 85 Glycine 80 75 76 70 Intensity % 65 60 55 50 D4-Alanine 45 40 35 13 172 15 C2 N-Glycine 30 25 126 186 153 79 94 20 135 178 15 10 5 0 50 100 150 m/z 200 250 300 Fig. 4: Amino acids profile for a case with MMA showing elevated glycine (m/z=76) and alanine (m/z=90). The study group included 3 patients (6%) who were asymptomatic at presentation and were suspected for OA because they had previous affected brothers or sisters.The 3 patients were later diagnosed for different types of OA. The neonatal period is the most critical period in the patient life when any metabolic crisis can be devastating and life threatening (Kamboj, 2008). Introducing the neonatal screening program, at least among the highly suspected families, will provide the early diagnosis and treatment and give those patients a chance for a better life. The effect of parental consanguinity was strongly observed in the study group. The majority of the study group (66%) were from consanguineous families.Also the number of similarly affected family members was much higher in consanguineous families; as a result,physicians should consider the possibility of the presence of genetic disorder. Consanguinity rates vary from one population to another depending on religion, culture, and geography.Temtamy and Loutife (1970) stated that the rate of consanguineous marriage among the Egyptian population was 33 %, while in another study carried out by Hafez et al (1983) it was 28.9 %. In a study made by Tadmouri et al in 2009, it was stated that many Arab countries, among which is Egypt, display some of the highest rates of consanguineous marriages in the world ranging around 20-50% of all marriages, and specifically favoring first cousin marriages with average rates of about 20-30%.This was attributed to socio-cultural factors, such as maintenance of family structure and property, ease of marital arrangements, better relations with inlaws, and financial advantages relating to dowry.The lack of awareness about the hazards of consanguineous marriage among Arab populations increases the rates of occurrence of genetic disorders. There is a persistent need for establishing screening programs in these countries to detect these increasing patients before they face their first metabolic attack with its resulting irreversible sequalae. The cost benefit relationship is obvious. Diagnosis of OA depends on the detection of organic acids in urine. The most common method for diagnosis of OA is GC/ MS analysis of the trimethylsilyl esters of the ethylacetate extract of organic acids in urine. (Sweetman, 1999). The aim of our work was to establish a rapid and accurate method for the diagnosis of patients suspected to have OA and to extend this method to be used for screening the high risk families. The use of Pitt`s method (Pitt et al., 2002) was sufficient especially that no quantitation was required. The results obtained by this method were compared to results of the same samples when analyzed using GC/ MS. The LC/ MS/ MS method offered the advantages of shorter run time (3 minutes compared to 75 min for GC/ MS), smaller sample size which is suitable for preterm and dehydrated patients and the use of samples without any drevatization. 1914 J. Appl. Sci. Res., 9(3): 1909-1916, 2013 Several organic acids could be detected in the study group and led to diagnosis of 31 patients with 11 different types of OA; We used Acylcarnitines and amino acids profiles for further confirmation (Table 1). Example for these OAs is methylmalonic acidemia(MMA) which was detected in 3 patients of the study group. Organic acids characteristic for this disorder (methylmalonate and 3-hydroxypropionate) could successfully be detected using LC/ MS/ MS (Fig 1) when compared to GC/ MS (Fig 2). Acylcarnitines profile showed elevated C3 acylcarnitine (Fig 3) and amino acids profile (Fig 4) showed elevated alanine and glycine, which confirmed the diagnosis. Methylmalonic acidemia is the most common OA in many studies (El Gammal et al., 2001; Selim et al., 2009). It was not the most common OA in our study but it had a frequency as high as 6% of the study group and 9.7% of the detected cases (Table 1). The MMA is disorder of branched chain amino acids metabolism. It results from either deficiency of the methylmalonyl CoA mutase enzyme or defect in the synthesis of its cofactor; Vit B12. Using our diagnostic approach couldn`t detect the underlying cause of MMA and measurement of enzyme activity or molecular studies is required if determination of the type is necessary. The most frequent diagnosed type of OA in the present study was maple syrup urine disease (MSUD); 6 cases were detected out of the 50 patients tested (12%) (Table 1). This is surprisingly high frequency in our population especially when compared to 2 previous studies made on Egyptian children in 2009, the 1st was done by Selim et al (2009)and didn`t detect any case with MSUD after screening 800 high risk patients, that is possibly because they first screened their patients using acylcarnitine profile and assayed organic acids only for patients showing abnormal acylcarnitine profiles which is not characteristic for MSUD patients. The 2nd study was done by Fateen et al(2009) who screened 117 high risk patients over 6 years and could detect only one case of MSUD. A larger study must be done on Egyptian children using samples taken from different regions of Egypt to know the different prevalent types of OA with their accurate frequencies. Glutarate, ethylmalonate, and methylsuccinate are three organic acids that are potential markers for many IEM, these compounds have the same parent mass (m/z 131) and daughter ions (m/z 87) when analyzed using LC/ MS/ MS, they couldn`t be distinguished by Pitt (2002) and was referred to as C5 dicarboxylate. We detected C5 dicarboxylic acid peaks in 4 patients of the study group (Table 1), to determine the type of OA; we looked for the simultaneously detected organic acids in each profile. In one of the patients, organic acids profile showed simultaneous accumulation of C4 dicarboxylate and lactate, this gave a possibility of multiple acyl CoA dehydrogenase deficiency (MADD). Acylcarnitines profiles confirmed the diagnosis by showing elevation of all acylcarnitines in the blood spot sample. In the other three patients, organic acids profile showed simultaneous accumulation of 3-hydroxyglutarate and the patients were diagnosed with Glutaric aciduria type I (GAI). Acylcarnitines profile confirmed the diagnosis by showing elevated C5DC Acylcarnitines. One of the patients diagnosed with GAI presented with intermittent form of the neurological manifestations. The organic acids profile using a random sample was normal, however, re-analyzing the patient using a sample taken during an acute attack revealed a pattern diagnostic for GAI. As a results, the possibility of OA shouldn`t be excluded before analyzing organic acids profile during an acute attack. Multiple carboxylase deficiency is an OA that was detected in 4 patients of the study group (8% of the study group & 13% of the diagnosed cases). The diagnosis depended on detection of variable organic acids and acylglycines (3-hydroxypropionate, 3-hydroxyisovalerate, C5:1 glycine and lactate) that couldn`t be assigned to a certain enzyme deficiency (Table 1). This condition is due to deficiency of either biotinidase or holocarboxylase synthetase involved in biotin metabolism (Burri et al., 1981). Our diagnostic approach couldn't determine which enzyme is deficient and the enzyme analysis must be done. The 4-hydroxyphenyllactate, 4-hydroxyphenylacetate and 4-hydroxyphenylpyruvate are 3hydroxyphenyldrevatives detected in the urine of 2 patients of the study groups (4% of the study group & 6.5% of the diagnosed cases) (Table 1). The detection of these compounds indicates the possibility of tyrosinemia; a disorder of tyrosine catabolism.Tyrosinemia has 3 clinically distinguished types; hereditary infantile tyrosinemia (tyrosinemia I; hepatorenal tyrosinemia), Richner-Hanhart syndrome (tyrosinemia II; occulocutaneous tyrosinemia), and tyrosinemia III (benign tyrosinemia).(Filiano, 2006). Using LC/MS/ MS in either detection of urinary hydroxyphenyl derivatives or in detection of blood tyrosine couldn`t assign the patients to a certain type of tyrosinemia. The patients were later diagnosed with tyrosinemia type I after detection of succinylacetone by GC/MS. Unfortunately, succinylacetone couldn`t be detected by LC/MS/ MS. Although both patients with tyrosinemia type I presented in the1st year of their lives which is not late for tyrosinemia I, they presented with so severe symptoms that they both died before the end of this study affected by complications of their disease.Both patients had severe anemia that is due to accumulation of succinylacetone. Anemia was also a result of diminished ability of the liver to produce clotting factors leading to severe bleeding. In a study made by Croffie et alin 1994, it was recommended that tyrosinemia type I be suspected in infants with severe bleeding even if there is no other signs of liver failure. 1915 J. Appl. Sci. Res., 9(3): 1909-1916, 2013 Orotic acid was detected in the urine of 3 patients of the study group (6% of the study group and10% of the diagnosed cases) (Table 1). The underlying cause of this orotic aciduria couldn`t be detected by the organic acids analysis alone. Because the treatment strategy depends on the type of orotic aciduria, the detection of amino acids in blood was necessary. In one of the patients with orotic aciduria, the amino acids profile was normal and it was attributed to a disorder of pyrimidine metabolism, a condition known as hereditary orotic aciduria. The treatment strategy was directed to administration of uridine. (Winkler and Suttle, 1988). In the other two cases, accumulated citrulline pointed to a secondary orotic aciduria that may be due to urea cycle defect. One case (2% of the study group) was detected for both mevalonic aciduria (MVA)and Methylglutaconic aciduria (MGA) (Table 1), both cases presented in the 1st year of their lives which is not a late age for their presentation. They didn`t show any characteristic clinical presentation except for the usual neurological symptoms and didn`t reveal any abnormal biochemical parameter. Organic acids profile was the only way for diagnosing both patients through detection of mevalonate for MVA and methylglutaconate for MGA. Although organic acids profiling could detect 3 cases of 2 fatty acid oxidation defects (MADD and MCADD), acylcarnitines profiling remains the most suitable method for detection of these disorder and must be used for confirmation of any patient with these defects detected by organic acids profiling. Conclusion: Egypt, like most other Arabian communities, is characterized by high rates of consanguineous marriages leading to widespread of genetic disorders among which are OAs. OA is a group of disorders that are greatly varied. They have no common clinical presentation or share the same biochemical abnormalities. Furthermore, these disorders are very aggressive, attack at a very young age and cause high morbidity and mortality rates in a very short time. Organic acid analysis is the only route for diagnosis of OA; this can be done using GC/MS or LC/ MS/ MS. Using LC/ MS/ MS in detection of urinary organic acids will facilitate introduction of neonatal screening program for OA, that is because it has a short run time thus can make large number of samples in a very short time and uses a small sample size that is suitable for neonatal period and preterm babies. However, LC/MS/ MS couldn`t detect some of the organic acids e.g. in case of succinylacetone, in this case, GC/MS can only be used. References Burri, B.J., L. Sweetman and W.L. Nyhan, 1981. Mutant holocarboxylase synthetase : Evidence for the enzyme defect in early infantile biotin responsive multiple carboxylase deficiency, J Clin Invest, 68: 1491-5. Croffie, J.M., S.K. Gupta, S.K.F. Chong and J.F. Fitzgerald, 1994. Tyrosinemia type I should be suspected in infants with severe bleeding with severe coagulopathy even in absence of other signs of liver failure, Pediatr Res., 35: 205-8. Dionisi-Vici, C., F. Deodato, W. Raschinger, W. Rhead and B Wilcken, 2006. Classical organic acidurias, propionic aciduria, methylmalonic aciduria, and isovaleric aciduria: Long-term outcome and effects of expanded newborn screening using tandem mass spectrometry,J Inherit Metab Dis, 29(2-3): 383-9. El Gammal, M.A., S.A. Temtamy, R. Shawky, M. Awadallah, M.S. Rashed, I Aboulezz, et al., 2001. Amino acid and organic acid disorders in 50 high risk Egyptian children. Egypt. J. Med. Hum. Genet., 2: 15-31. Fateen, E., A. Gouda, H. Boehles and A Sewell, 2009. Inborn errors of metabolism revealed by organic acid profile analysis in high risk egyptian patients: Six years experience, Egypt J Med Hum Genet, 10(2): 18697. Filiano, J.J., 2006. Neurometabolic diseases in the newborn. ClinChim, 3(2): 411-79. Hafez, M., H. El Tahan, M. Awadalla, H. El Khayat, A. Abdel Gafar and M. Ghneim, 1983. Consanguineous mating in the Egyptian population, J Med Genet, 20: 58-60. Hoffmann, G.F., 1994. Selective screening for inborn errors of metabolism past, present and future, Eur J Pediatr, 153(7 suppl 1): S2-8. Hori, D., Y. Hasegawa, M. Kimura, Y. Yang, I.C. Verma and S. Yamaguchi, 2005. Clinical onset and prognosis of Asian children with organic acidemias, as detected by analysis of urinary organic acids using GC/MS, instead of mass screening. Brain Dev., 27(1): 39-45. Kamboj, M., 2008. Clinical approach to the diagnosis of inborn errors of metabolism, Pediatr Clin North Am, 55: 1113-27. Keeratichameron, S., J.R. Cairn, P. Sawangareetrakul, S. Liammongkolkul, V. Champattanachai, C. Srisomsap, et al., 2005. Novel mutations found in two genes of thai patients with isolated methylmalonic academia. Biochem. Genet., 45(5-6): 421-30. 1916 J. Appl. Sci. Res., 9(3): 1909-1916, 2013 Pitt, J.J., M. Eggington and S.G. Kahler, 2002. Comprehensive screening of urine samples for inborn errors of metabolism by electrospray tandem mass spectrometry. ClinChem, 48: 1970-80. Schulze, A., M. Lindner, D. Kohlmuller, K. Olgemeller, E. Mayatepek and G.F. Hoffmann, 2003. Expanded newborn screening for inborn errors of metabolism by electrospray ionization – tandem mass spectrometry: Results, outcome, and implications, Pediatrics, 111(6): 1399-1406. Selim, L., S. Hassan, F. Salem, F. Hassan, F. El Mogy, S. Abdel Atty, I. Mandour, M. Fathy, A. Amin, I. Gamal el din, M. El defrawy, A. El ayat, A. El Badawy, M. Yousry, M. Abdel Monem and D. Mehaney, 2009. Screening for organic acid disorders among Egyptian children with clinically suspected neurometabolic disease, Research Journal for Medicine and Medical Science, 4(2) (2009):369-85. Sweetman, L., 1999. Organic acid analysis. In: Techniques in diagnostic human biochemical genetics. Hommes FA (Ed). A laboratory manual: Wiley-Liss, pp: 143. Tadmouri, G.O., P. Nair, T. Obeid, M.T. Al Ali; N. Al Khajaand H.A. Hamamy, 2009. Consanguinity and reproductive health among Arabs, Reproductive health, 6:17. Tanaka, K., M.A. Budd, M.L. Efron and K.J. Issel-bacher, 1966. Isovaleric acidemia: A new genetic defect of leucine metabolism,Proc.Natl. Acad. Sci. U.S.A., 56(1): 236-42. Temtamy, S.A., A.H. and Loutfi, 1970. Some genetic and surgical aspects of the cleft lip-palate problem in Egypt, Cleft Palat J., 7: 578-94. Wajner, M., M. Coelho Dde, R. Ingrassia, A.B. de Oliveira, E.N. Busarrelo, K. Raymond, et al., 2009. Selective screening for organic acidemias by urine organic acids GC-MS analysis in Brazil: Fifteen-year experience, Clin. Chim. Acta., 400(1-2): 77-81. Wasant, P., S. Liammongkolkul, C. Kuptanon, N. Vatanavicharn, A Sathienkijakanchai and T. Shinka, 2008. Organic acid disorders detected by urine organic acid analysis: Twelve cases in Thailand over three-year experience, Clin. Chim. Acta., 392(1-2): 63-8. Winkler, J.K. and D.P. Suttle, 1988. Analysis of UMP synthase gene and mRNA structure in hereditary orotic aciduria fibroblasts. Am J Hum Genet, 43(1): 86-94. Zoppa, M., L. Gallo, F. Zacchello and G. Giordano, 2006. Method for the quantification of underivatized amino acids on dry blood spots from newborn screening by HPLC–ESI–MS/MS,Journal of Chromatography B, 831(1-3): 267-73.