Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
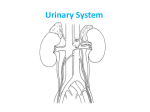
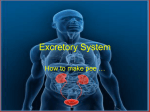
Chapter 26 The Urinary System Three major functions: excretion: removal of organic wastes from body fluids elimination: discharge of waste products into the environment regulate blood plasma: volume and solute concentration Major organs kidneys (2) produce urine water, soluble compounds urinary tract: ureters (2) kidney to urinary bladder urinary bladder (1) temporary storage of urine urethra (1) urinary bladder to exterior Other important functions: regulate blood volume and pressure regulate [ions] in blood Na+, K+, Cl-, etc., stabilize blood pH conserve nutrients while getting rid of wastes detoxify compounds kidney location fig. 26-2 fig. 26-2a The Kidneys location on either side of vertebral column around T12 to L3 capped by adrenal gland retroperitoneal supported by CT surrounded by adipose (cushioning) to here 4/4/07 lec# 35 The Kidneys anatomy: hilum indentation entry/exit ureters renal artery, vein, nerves fig. 26-4a The Kidneys anatomy: renal cortex renal medulla renal pyramids minor calyx major calyx renal pelvis nephrons tubular functional numerous vascular The Kidneys blood supply 20-25% of cardiac output renal artery segmental artery interlobar artery arcuate artery kidney vasculature fig. 26-5a fig. 26-5a The Kidneys blood supply coming off of arcuate arteries interlobular arteries afferent arteriole glomerulus efferent arteriole peritubular capillary interlobular veins arcuate veins fig. 26-5a The nephron overview renal corpuscle renal tubule renal tubule fig 26-6 renal corpuscle The nephron: parts Bowman’s capsule loop of Henle distal convoluted tubule fig. 26-6a Bowman’s capsule dct pct loop of Henle proximal convoluted tubule fig. 26-9 The nephron: blood supply efferent arteriole glomerulus (capillary bed) afferent arteriole fig. 26-6a ? The nephron: blood supply peritubular capillaries efferent arteriole glomerulus (capillary bed) afferent arteriole fig. 26-6a The nephron: Bowman’s capsule hollow structure two layers visceral (inner) parietal (outer) surrounds glomerulus fig 26-6a The nephron: Bowman’s capsule fig. 26-8 What is between blood and space? podocytes and filtration slits lamina densa (connective tissue) fenestrated endothelium (capillary) pedicel pedicel podocyte 1 filtration slits podocyte 2 The nephron: Bowman’s capsule fig. 26-8 endothelium lamina densa filtration slits blood capsular space = filtration membrane fig. 26-10 blood pressure forces water and small solutes across “membrane” into Bowman’s capsule fig. 26-10 wastes but also water glucose amino acids vitamins fatty acids etc. = glomular filtrate fig. 26-10 but not: cells large plasma proteins fig. 26-10 The nephron: proximal convoluted tubule proximal convoluted tubule fig. 26-6a pct The nephron: proximal convoluted tubule cuboidal cells microvilli reabsorption remove water, nutrients etc., from the glomerular filtrate and release them into the peritubular fluid loop of Henle fig. 26-6a loop of Henle The nephron: loop of Henle The nephron: loop of Henle descending limb thick pumps Na+ Cl- out of fluid thin permeable to H2O ascending limb thin thick The nephron: distal convoluted tubule dct distal convoluted tubule fig. 26-6a The nephron: distal convoluted tubule active secretion (ions, acids, drugs) selective reabsorption of Na+ and Ca2+ selective reabsorption of H2O The nephron: distal convoluted tubule also part of the jg apparatus (JGA) (juxtaglomerular) macula densa (DCT) juxtaglomerular cells (afferent arteriole) secrete EPO, renin juxtaglomerular apparatus The collecting system DCT collecting duct papillary duct minor calyx … 100 keys (pg. 959) “The kidneys remove waste products from the blood; they also assist in the regulation of blood volume and blood pressure, ion levels, and blood pH. Nephrons are the primary functional units of the kidneys.” Renal Physiology what is the kidney doing how does it accomplish these tasks Goal regulate volume and composition of the blood involves excretion of wastes Renal Physiology three major organic wastes urea 21g / day from amino acid breakdown creatinine 1.8 g / day from CP breakdown uric acid 480 mg / day recycling RNA N-bases Renal Physiology three major organic wastes can be eliminated only when dissolved in urine (H2O loss) production of hyperosmotic urine restrict excessive H2O loss reabsorb useful molecules Renal Physiology: steps 1. filtration blood pressure forcing water and small solutes (good and bad) from capillaries into capsular space Renal Physiology: steps 2. reabsorption remove water and many solutes from filtrate by: diffusion, osmosis channel-mediated diffusion carrier-mediated transport Renal Physiology: steps 2. reabsorption many different proteins involved a cell may have many functions differential distribution of proteins transport can be saturated Renal Physiology: steps 3. secretion transport of solutes from body fluids into the tubular fluid (or filtrate) table 26-2 to here 4/11/07 lec# 36 Filtration filtration membrane lets water and small solutes through cells and plasma proteins stay in capillaries 100 keys (pg. 969) “Roughly 180 L of filtrate is produced at the glomeruli each day, and that represents 70 times the total plasma volume. Almost all of that fluid volume must be reabsorbed to avoid fatal dehydration.” Filtration: hydrostatic pressure glomerular hydrostatic pressure (GHP) push fluid out of vessels (bp) capsular hydrostatic pressure (CsHP) push fluid back into vessels net hydrostatic pressure (NHP) NHP = GHP - CsHP 35 = 50 - 15 mm Hg Filtration: colloid pressure blood colloid osmotic pressure (BCOP) proteins in blood (hyperosmotic) draw water back into blood ~ 25 mm Hg Filtration: filtration pressure (FP) FP = NHP - BCOP 10 = 35 - 25 mm Hg importance of blood pressure 20% drop in blood pressure 50mm Hg to 40mm Hg filtration would stop Filtration: filtration rate (GFR) glomerular filtration rate (GFR) amount of fluid pushed into the capsular space each minute GFR ~ 125 ml / min 180 liters (~50 gallons)/ day Filtration: filtration rate (GFR) affected by filtration pressure (FP) change FP change GFR significant factor in FP is… … blood pressure Filtration: filtration rate (GFR) control of GFR adequate blood flow to glomerulus adequate filtration pressure autoregulation hormonal regulation autonomic regulation Filtration: filtration rate (GFR) autoregulation lower bp afferent arteriole glomerulus efferent arteriole dilate dilate constrict Filtration: filtration rate (GFR) autoregulation higher bp afferent arteriole contract less blood in lower GHP Filtration: filtration rate (GFR) hormonal regulation renin-angiotensin system renin is released when: drop in bp JG cells stimulated by sym. lower osmolarity of tubular fluid Filtration: filtration rate (GFR) hormonal regulation bp renin angiotensin II bp constrict afferent art. secretion of aldosterone thirst secretion of ADH general vasoconstriction Filtration: filtration rate (GFR) hormonal regulation bp GFR fluid loss bp ANP BNP GFR Na+ reabsorption urine production fig. 26-11 Filtration: filtration rate (GFR) autonomic (ANS) regulation bp sympathetic stimulation powerful vasoconstriction of afferent arteriole GFR bp Filtration: filtration rate (GFR) maximal physical exertion (ie., marathon, etc.,) blood to muscle less blood to kidney damage to glomerulus proteinuria hematuria Renal Physiology: reabsorption/secretion PCT reabsorbs 60-70% of filtrate peritubular fluid peritubular capillaries Renal Physiology: reabsorption/secretion PCT reabsorb organic nutrients active reabsorption of ions reabsorption of H2O passive reabsorption of ions secretion Renal Physiology: reabsorption/secretion PCT reabsorb organic nutrients 99% absorbed before reaching the loop of Henle facilitated transport cotransport (carrier proteins) Renal Physiology: reabsorption/secretion PCT active reabsorption of ions Na+ K+ HCO3- active transport (carrier proteins and ATP) Renal Physiology: reabsorption/secretion PCT reabsorption of H2O filtrate solutes H 2O fig. 26-12 Renal Physiology: loop of Henle countercurrent exchange (multiplication) fluids moving in opposite directions descending limb ascending limb Renal Physiology: loop of Henle thin descending limb permeable to H2O impermeable to solutes thick ascending limb impermeable to both contains Na+ + Cl- pumps Renal Physiology: loop of Henle thick ascending limb contains Na+ + Cl- pumps pumps ions out of the tubular filtrate into the peritubular fluid makes peritubular fluid hyperosmotic ascending limb is not permeable, but has pumps Na+-K+/2Cltransporter fig 26-13 Na+-K+/2Cltransporter fig 26-13a Renal Physiology: loop of Henle thick ascending limb contains Na+ + Cl- pumps makes peritubular fluid hyperosmotic as thin, descending limb passes down, H2O diffuses out making fluid more concentrated permeable to H20, not solutes fig 26-13 which means there are more ions to pump out that makes tubular fluid more concentrated positive feedback maintains a hyperosmotic peritubular fluid sets up a concentration gradient within the medulla of the kidney papillary duct is only place permeable to urea to here 4/13 lec # 37 Renal Physiology: distal convoluted tubule only 15-20% of original volume of filtrate makes it to the DCT final adjustments are made here: reabsorption secretion Renal Physiology: distal convoluted tubule reabsorption remove Na+ and Cl- from filtrate aldosterone stimulates the Na+ pumps in some parts of the DCT fig. 26-14 Renal Physiology: distal convoluted tubule secretion K+ sodium-potassium exchange H+ secreted to raise blood pH HCO3- is produced (buffer blood) fig. 26-14c Renal Physiology: the collecting system reabsorption and secretion collecting ducts gather tubular fluid from many nephrons and transport it toward the ureter through the concentration gradient set up in the medulla Renal Physiology: the collecting system regulation aldosterone activate Na+ pumps of DCT and collecting duct ADH controls permeability of collecting duct to H2O Renal Physiology: the collecting system reabsorption Na+ aldosterone controlled exchange for K+ Bicarbonate exchange for ClUrea usually diffuses out of lower portion of collecting duct Renal Physiology: the collecting system secretion can secrete H+ to raise pH or bicarbonate to lower pH 100 keys (pg. 976) “Reabsorption involves a combination of diffusion, osmosis, channel-mediated diffusion, and active transport. Many of these processes are independently regulated by local or hormonal mechanisms. the primary mechanism governing water reabsorption can be described as “water follows salt.” Secretion is a selective, carrier-mediated process.” What happens to all that stuff that has been reabsorbed and put into the peritubular space? taken up by the peritubular capillaries and returned to circulation. Control of water reabsorption will determine: volume of urine osmotic concentration of urine Control of water reabsorption 85% will occur no matter what PCT descending limb of loop of Henle osmosis Control of water reabsorption remaining 15% is reabsorbed (or not) by the DCT and the collecting duct (27 L / day) Control of water reabsorption DCT and the collecting duct are usually impermeable to H2O except in the presence of ADH no ADH more, dilute urine fig. 26-15 with ADH less, concentrated urine Control of water reabsorption diabetes insipdus underproduction of ADH not enough water reabsorbed (too much water lost) Control of water reabsorption diabetes insipdus flow through >10 liters of urine / day very thirsty tasteless Control of water reabsorption ANP BNP natriuretic peptides oppose action of ADH Diuretics: drugs that promote H2O loss reduce blood volume blood pressure ECF Normal Urine clear sterile yellow odorous no bacteria urobilin pigment evaporation of small molecules ammonia etc., ketones ? urinalysis color, appearance, taste, chemical summary fig. 26-16 Urine transport, storage and elimination fig. 26-7a fig. 26-4a Urine transport, storage and elimination collecting duct minor calyx major calyx renal pelvis ureter fig. 26-17 Urine transport, storage and elimination ureter urinary bladder fig. 26-18c Urine transport, storage and elimination ureter urinary bladder sphincters (2) urethra urethral opening Urine transport, storage and elimination fig. 26-18 Urine transport, storage and elimination fig. 26-18 Urine transport, storage and elimination micturation reflex 1. stretch bladder 2. sense 3. stimulate muscle 4. relax sphincter(s) Urine transport, storage and elimination micturation reflex incontinence inabililty to voluntarily control urination Aging and the urinary system 1. decline in # of functional nephrons 2. reduction in GFR (#1, reduced blood flow) 3. less responsive to ADH 4. voiding problems loss of muscle tone cerebral damage bph