Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
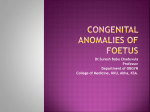
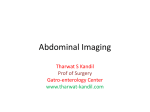
Archives of Cardiovascular Disease (2014) 107, 4—9 Available online at ScienceDirect www.sciencedirect.com CLINICAL RESEARCH Real-time three-dimensional foetal echocardiography using a new transabdominal xMATRIX array transducer Échocardiographie cardiaque fœtale 3D temps réel par voie trans-abdominale avec une nouvelle sonde matricielle Philippe Acar a,∗, Laia Battle b, Yves Dulac a, Marianne Peyre a, Hélène Dubourdieu b, Sébastien Hascoet a, Marion Groussolles b, Christophe Vayssière b a Department of Paediatric Cardiology, Children’s Hospital, 330, avenue de Grande-Bretagne, 31059 Toulouse cedex 9, France b Department of Obstetrics and Gynaecology, Mother’s Hospital, Toulouse, France Received 5 August 2013; received in revised form 18 October 2013; accepted 24 October 2013 Available online 22 December 2013 KEYWORDS Fetal echocardiography; 2D echocardiography; 3D echocardiography; Congenital heart defect; STIC Summary Background. — Foetal echocardiography has been used to diagnose congenital heart disease. However, conventional echocardiography can only display two-dimensional (2D) structural images of the intricate three-dimensional (3D) foetal heart. Aim. — The purpose of this study was to report the first use of a new transabdominal xMATRIX array transducer and to describe its ability to perform all 3D modalities: intelligent spatiotemporal image correlation (iSTIC) acquisition, xPlane imaging and 3D surface imaging. Methods. — Eighty foetuses without congenital heart disease were included consecutively, with a gestational age between 20 and 37 weeks. 2D and 3D scans were performed with a transabdominal xMATRIX array transducer. Cardiac-STIC volume datasets were acquired and postprocessed with new automatic software (the ‘Fetal Heart Navigator’). Results. — A total of 224 iSTIC acquisitions were performed (mean time for each, 2 seconds). Only 78 iSTIC acquisitions (35%) were able to detect the ductal arch automatically. ‘Fetal Heart Navigator’ feasibility varied according to foetal position, including the descending aorta. Live Abbreviations: 2D, two-dimensional; 3D, three-dimensional; CHD, congenital heart disease; FHN, ‘Fetal Heart Navigator’; iSTIC, intelligent spatiotemporal image correlation; STIC, spatiotemporal image correlation. ∗ Corresponding author. E-mail address: acar.p@chu-toulouse.fr (P. Acar). 1875-2136/$ — see front matter © 2013 Elsevier Masson SAS. All rights reserved. http://dx.doi.org/10.1016/j.acvd.2013.10.003 Real-time 3D foetal echo 5 xPlane imaging had excellent feasibility regardless of foetal position; using rotation, lateral and vertical tilts, all cardiac structures were identified from a unique reference plane. Live 3D surface imaging had variable feasibility depending on the target structure. Only 10% of the volume dataset offered comprehensive imaging of intracardiac views. Conclusion. — The new xMATRIX transabdominal transducer allows a multimodality approach to the foetal heart. Further studies that include foetuses with cardiac malformations are required. © 2013 Elsevier Masson SAS. All rights reserved. MOTS CLÉS Échocardiographie fœtale ; Échocardiographie 2D ; Échocardiographie 3D ; Cardiopathie congénitale ; STIC Résumé Contexte. — L’échocardiographie fœtale permet de dépister les malformations cardiaques chez le fœtus. Néanmoins, les ultrasons conventionnels sont limités à des coupes 2D. Objectif. — Notre but a été de rapporter la 1re utilisation d’une sonde matricielle 3D transabdominale chez le fœtus. Méthodes. — Quatre-vingt fœtus sans malformations cardiaque d’âge gestationnel de 20 à 37 semaines d’aménorrhée ont été inclus incluant des acquisitions 2D et 3D (iSTIC, xPlan et imagerie de surface 3D). Un nouveau processeur automatique des données STIC (fetal heart navigator) a été utilisé. Résultats. — Deux cent vingt-quatre acquisitions iSTIC ont été réalisées (temps moyen de deux secondes). Seulement 78 acquisitions iSTIC (35 %) ont été exploitables par le fetal heart navigator (nécessité d’inclure l’aorte descendante). Le xPlan avait une bonne faisabilité indépendante de la position du fœtus. À partir d’une image de référence, après rotation ou inclinaison latérale et verticale tilts, toutes les structures cardiaques ont pu être identifiées. L’imagerie de surface 3D n’a donné une image exploitable que dans 10 % des fœtus. Conclusion. — La nouvelle sonde matricielle xMATRIX transabdominale permet une approche multimodale du cœur fœtal. D’autres études sont nécessaires pour démontrer son intérêt dans le dépistage des malformations cardiaques. © 2013 Elsevier Masson SAS. Tous droits réservés. Background Congenital heart disease (CHD) is one of the most common congenital anomalies and is the leading cause of neonatal and infant mortality. Prenatal diagnosis of CHD has benefits for parental counselling, decision making during pregnancy, prenatal interventions, site and mode of delivery, and postnatal management [1]. The detection rate of prenatal cardiac lesions has increased significantly during the past two decades with the improvement in foetal echocardiography [2]. Two-dimensional (2D) foetal echocardiography has been used to screen, diagnose, monitor and treat congenital heart defects and rhythm abnormalities [3]. However conventional echocardiography can only display 2D structural images of the intricate three-dimensional (3D) foetal heart. 3D echocardiography has been shown to enhance the diagnosis of CHD in children [4,5]. Spatiotemporal image correlation (STIC) was first introduced for 3D foetal echocardiography using mechanical transducers [6,7]. STIC acquires a series of volume data that can be displayed in any plane. However, postprocessing of the volume dataset requires expertise [8,9]. Real-time 3D echocardiography in the foetus was recently introduced with the development of the cardiac xMATRIX array transducer [10,11]. This type of transducer enables visualization and examination of the pulsating foetal heart in real time, without the need for gating, and is unaffected by motion artefacts. Live 3D surface and xPlane imaging are modalities of this new technology [12]. However, STIC and live 3D imaging have never been produced by the same ultrasound system. We report for the first time on a new transabdominal xMATRIX array transducer. Our aim was to describe its ability to perform the three modalities of 3D imaging: STIC acquisition, xPlane imaging and 3D surface imaging. New automatic software for displaying STIC planes was tested. Methods Eighty women with singleton pregnancies (gestational age between 20 and 37 weeks) were studied consecutively at Toulouse University Hospital from July to October 2012. All patients had undergone previous 2D ultrasound examinations that excluded any malformations. Informed consent was obtained in all cases. Transabdominal real-time 3D echocardiography was performed using an iU22 ultrasound machine (Philips Medical Systems, Bothell, WA, USA) equipped with an x6-1 PureWave xMATRIX array transducer (Fig. 1). All 3D echocardiography was performed by two experienced operators (P.A. and C.V.). Three modalities of 3D imaging were performed. Intelligent STIC (iSTIC) acquisition With the full volume angle set at 20◦ and an acquisition time of only 3 seconds, this fast acquisition is obtained thanks to the electronic phasing of the x6-1 xMATRIX transducer (versus 10 seconds with the conventional STIC method on a mechanical transducer). The acquisition was started from a four-chamber view during a foetal quiescent period. Two to three sets of volume data were collected for each case 6 P. Acar et al. and saved on the hard disk of the machine. All volume datasets were analysed off-line using dedicated software by two independent observers (L.B. and M.G.). Postprocessing was performed using the ‘Fetal Heart Navigator’ (FHN) software (plug-in within QLAB 9.0 software; Philips Medical Systems, Bothell, WA, USA; 2011). The FHN software automatically detects the ductal arch as the initial view no matter what position the iSTIC data set or STIC data set is acquired in (Fig. 2). For the next step, the user was guided in obtaining the views recommended by the ISUOG guidelines on foetal cardiac screening: the four-chamber view and the left and right ventricular outflow tract views [3]. At the end of the protocol, all four views were displayed on one screen. Figure 1. x6-1 PureWave xMATRIX array transducer containing 9000 active elements (35 times more elements than conventional transducers), allowing different imaging modes, such as iSTIC acquisition, live xPlane imaging and live 3D imaging. Live xPlane imaging The xMATRIX array transducer allows the simultaneous display by using a split-screen format of two high-resolution real-time views: a primary reference imaging plane and a secondary imaging plane selected by electronic rotation of the ultrasound beam (Fig. 3). A rotation through a full 360◦ Figure 2. A. ‘Fetal Heart Navigator’: acquisition with the x6-1 xMATRIX array transducer on the iU22 ultrasound system (Philips Medical Systems, Bothell, WA, USA) on the normal heart of a 24-week foetus. Extraction of the four-chamber view (1), left ventricular outflow tract (2), right ventricular outflow tract (3) and ductal arch (4). B. ‘Fetal Heart Navigator’: acquisition with the x6-1 xMATRIX transducer on the iU22 ultrasound system on the normal heart of a 30-week foetus. The system cannot find the required ductal arch view. Real-time 3D foetal echo 7 Figure 4. Live 3D imaging with the x6-1 xMATRIX array transducer on the iU22 ultrasound system (Philips Medical Systems, Bothell, WA, USA) of the normal heart of a 30-week foetus. Extraction of the four-chamber view in a volume. Analysis was performed by two independent observers (Y.D. and S.H.). Results Figure 3. A. xPlane with lateral tilt selected of the normal heart of a 30-week foetus. Left image (the acquisition view): ventricular short-axis view. Right image: real-time lateral view (scan plane demonstrated by the white line bisecting the left view). B. xPlane with lateral tilt selected of the normal heart of a 20-week foetus. Left image (the acquisition view): right ventricular outflow tract. Right image: real-time lateral extraction view, showing the left ventricular outflow tract (demonstrated by the white line bisecting the left image). was applied from the reference image plane. A lateral tilt from −45◦ to +45◦ was added to the rotated image plane. From the reference plane, an elevation tilt was performed from −30◦ to +30◦ . Live 3D surface imaging The system acquired 3D data using a 40◦ × 20◦ pyramidal imaging volume of the target organ (Fig. 4). Two orthogonal reference planes were used to localize cardiac structures in the volume. Navigation by cropping inside the volume allowed surface rendering of the intracardiac structures. A total of 224 iSTIC acquisitions were performed in 80 foetuses. The mean time for each acquisition with the xMATRIX array transducer was 2 seconds. All the volume datasets were analysed using the FHN software. We defined the feasibility of the FHN as the ability to depict the ductal arch view from the initial acquisition. Only 78 iSTIC acquisitions were able to detect the ductal arch automatically, resulting in a feasibility of 34.8% for FHN. Feasibility varied according to foetal position (either apical, right-sided or left-sided insonation of the four-chamber view of the foetal heart), including the descending aorta. Live xPlane imaging had excellent feasibility (95%) regardless of foetal position. Using rotation, lateral and elevation (vertical) tilts, all normal cardiac structures were identified from a unique reference image plane: the atrial cavity and septum; the atrioventricular valves; the ventricular cavity and septum; the left and right ventricular outflow tracts; the ascending aorta; and the main pulmonary artery and its bifurcation. The feasibility of live 3D surface imaging varied depending on the target structure. Only 10% of the volume dataset offered comprehensive imaging. By cropping and rotating the 3D pyramid, intracardiac en face views of the atrioventricular valves were obtained, including dynamic motion. Discussion This is the first report using a transabdominal xMATRIX array transducer applying all modalities of 3D imaging to the foetal 8 heart: STIC acquisition, xPlane imaging and 3D surface imaging. iSTIC acquisition and postprocessing STIC was first introduced for 3D foetal echocardiography in 2003 using mechanical transducers [6]. STIC is an automated volume acquisition in which the array inside the transducer performs a slow single sweep, recording a 3D volume dataset. The major limitations of STIC technology acquired with mechanical transducers are that the image is not acquired in real time, making foetal movement a problem during the acquisition time [7—9]. Such motion can generate some degradation in image quality from the 2D image. Here, we report the first study of iSTIC acquisition performed using an electronic xMATRIX array transducer. We acquired a high-resolution loop of volumes over a foetal cardiac cycle in only 2 seconds (as opposed to 10 seconds with conventional STIC), unaffected by motion artefacts. Whatever the mode of STIC or iSTIC acquisition, the acquired volume dataset needs off-line re-examination. Postprocessing of the volume dataset requires time and expertise. We used new protocol-driven workflow FHN software. It does not matter in which position the iSTIC or STIC data set is acquired for the FHN software. A major limitation of the software is the difficulty in detecting the ductal arch (dependent on the foetal position and the acquisition box). Feasibility could be increased by using right-sided or leftsided insonation of the four-chamber view of the foetal heart, including the descending aorta. However by following the ISUOG guidelines, the FHN should simplify foetal heart examination from the STIC volume [3]. Even if STIC modalities have limited value in the foetal diagnosis of CHD, many studies have reported its usefulness in assessing cardiac function, atrial morphology, vessels and atrioventricular valve measurements [13—16]. STIC by telemedicine is also a promising modality [17]. The advantage of the xMATRIX array transducer comes from its ability to switch to other 3D modalities, such as live xPlane and 3D surface rendering. Live xPlane imaging Whereas a conventional 2D foetal echocardiogram typically requires several minutes to obtain multiple views from different sweeps, xPlane imaging is a new mode that allows a total scan of the foetal heart without moving the transducer. Live xPlane imaging (or ‘biplane imaging’) is the scanning of two image planes of the foetal heart at different angles. The Live xPlane imaging technique does not require cardiac monitoring of the foetal cardiac cycle and avoids the potential artefacts produced by the cardiac gating method. Use of this method to display two cardiac planes simultaneously — namely, the four-chamber and ventricular outflow planes — without needing to move the transducer, has been previously described [10,18]. The rotation angle depends on the position of the foetal heart and on the normality of the outflow tract. Xiong et al. reported a live xPlane imaging study in the foetus to visualize simultaneously the four-chamber and inplane views of the interventricular septum; they concluded P. Acar et al. that this method may be a useful tool for the assessment of ventricular septal defects [19]. In our study, live xPlane imaging was able to identify a normal foetal heart with a single position of the transducer, despite the foetus being in a difficult position, even if we only used the lateral xPlane view and the elevation mode available on the xMATRIX system. Live 3D surface imaging Live 3D surface imaging provides real-time volumetric examination of the target organ. 3D volume rendering provides unique views of cardiac anatomical structures, which are not easily understood on conventional 2D imaging. The use of live 3D surface imaging has been extensively reported in paediatric and adult cardiology; it has been shown to be particularly useful in the assessment of valvular diseases and CHD [4,5]. Studies using live 3D surface imaging in foetal echocardiography are still limited. We and others previously reported that using a cardiac xMATRIX array transducer for 3D surface imaging could more precisely describe the size of patent foramen ovale as well the location of intracardiac tumours [10,20]. Using the same xMATRIX transducer, Xiong et al. reported the ability of the en face view of the interventricular septum to better visualize ventricular septal defect in the foetus [21]. However, this imaging is limited by the low penetration of the high-frequency transducer as well as the narrow scanning angle [22]. Further studies are necessary to explore the role of this new xMATRIX transabdominal transducer in foetal echocardiography. Our study is the first report of live 3D surface imaging using the transabdominal xMATRIX transducer. Volume scans are less dependent on the angle of acquisition, which means that obtaining the requisite data may be dependent on foetal lie or operator expertise. As the resolution of real-time 3D volume display remains inferior to that of conventional 2D imaging, its application in foetal echocardiography is still limited [10,12—24]. Further studies are required to compare the abilities of 3D versus 2D in foetuses that are challenging, in terms of acoustic window and foetal position. Moreover, these studies should include foetuses with cardiac malformations. As this sentence speaks to the cardiac xMATRIX transducer. Can we suggest to move it up to the position indicated Before the sentence starting with ‘‘Further studies are necessary’’. Disclosure of interest The authors declare that they have no conflicts of interest concerning this article. Acknowledgments Philips loaned an iU22 xMATRIX ultrasound system to the prenatal department of the University Hospital of Toulouse. Real-time 3D foetal echo References [1] Bonnet D, Coltri A, Butera G, et al. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation 1999;99:916—8. [2] Allan L. Antenatal diagnosis of heart disease. Heart 2000;83:367. [3] Rychik J, Ayres N, Cuneo B, et al. American Society of Echocardiography guidelines and standards for performance of the fetal echocardiogram. J Am Soc Echocardiogr 2004;17:803—10. [4] Acar P, Abadir S, Paranon S, et al. Live 3D echocardiography with the pediatric matrix probe. Echocardiography 2007;24:750—5. [5] Acar P, Saliba Z, Bonhoeffer P, et al. Influence of atrial septal defect anatomy in patient selection and assessment of closure with the Cardioseal device; a three-dimensional transoesophageal echocardiographic reconstruction. Eur Heart J 2000;21:573—81. [6] Goncalves LF, Lee W, Chaiworapongsa T, et al. Four-dimensional ultrasonography of the fetal heart with spatiotemporal image correlation. Am J Obstet Gynecol 2003;189:1792—802. [7] Uittenbogaard LB, Haak MC, Spreeuwenberg MD, et al. A systematic analysis of the feasibility of four-dimensional ultrasound imaging using spatiotemporal image correlation in routine fetal echocardiography. Ultrasound Obstet Gynecol 2008;31:625—32. [8] Bennasar M, Martinez JM, Gomez O, et al. Accuracy of four-dimensional spatiotemporal image correlation echocardiography in the prenatal diagnosis of congenital heart defects. Ultrasound Obstet Gynecol 2010;36:458—64. [9] Wanitpongpan P, Kanagawa T, Kinugasa Y, et al. Spatio-temporal image correlation (STIC) used by general obstetricians is marginally clinically effective compared to 2D fetal echocardiography scanning by experts. Prenat Diagn 2008;28:923—8. [10] Acar P, Dulac Y, Taktak A, et al. Real-time three-dimensional fetal echocardiography using matrix probe. Prenat Diagn 2005;25:370—5. [11] Sklansky MS, DeVore GR, Wong PC. Real-time 3-dimensional fetal echocardiography with an instantaneous volumerendered display: early description and pictorial essay. J Ultrasound Med 2004;23:283—9. [12] Xiong Y, Chen M, Chan LW, et al. Scan the fetal heart by real-time three-dimensional echocardiography with live xPlane imaging. J Matern Fetal Neonatal Med 2012;25: 324—8. 9 [13] Godfrey ME, Messing B, Valsky DV, et al. Fetal cardiac function: M-mode and 4D spatiotemporal image correlation. Fetal Diagn Ther 2012;32:17—21. [14] Luewan S, Yanase Y, Tongprasert F, et al. Fetal cardiac dimensions at 14—40 weeks’ gestation obtained using cardio-STIC-M. Ultrasound Obstet Gynecol 2011;37:416—22. [15] Paladini D, Sglavo G, Masucci A, et al. Role of four-dimensional ultrasound (spatiotemporal image correlation and sonographybased automated volume count) in prenatal assessment of atrial morphology in cardiosplenic syndromes. Ultrasound Obstet Gynecol 2011;38:337—43. [16] Yagel S, Cohen SM, Rosenak D, et al. Added value of three-/four-dimensional ultrasound in offline analysis and diagnosis of congenital heart disease. Ultrasound Obstet Gynecol 2011;37:432—7. [17] Adriaanse BM, Tromp CH, Simpson JM, et al. Interobserver agreement in detailed prenatal diagnosis of congenital heart disease by telemedicine using four-dimensional ultrasound with spatiotemporal image correlation. Ultrasound Obstet Gynecol 2012;39:203—9. [18] Yuan Y, Leung KY, Ouyang YS, et al. Simultaneous real-time imaging of four-chamber and left ventricular outflow tract views using xPlane imaging capability of a matrix array probe. Ultrasound Obstet Gynecol 2011;37:302—9. [19] Xiong Y, Wah YM, Chen M, et al. Real-time three-dimensional echocardiography using a matrix probe with live xPlane imaging of the interventricular septum. Ultrasound Obstet Gynecol 2009;34:534—7. [20] Hata T, Kanenishi K, Tanaka H, et al. Real-time 3-D echocardiographic evaluation of the fetal heart using instantaneous volume-rendered display. J Obstet Gynaecol Res 2006;32:42—6. [21] Xiong Y, Wah YM, Chen M, et al. Assessment of the fetal interventricular septum using real-time three-dimensional echocardiography with Live 3D imaging. Ultrasound Obstet Gynecol 2010;35:754—5. [22] Maulik D, Nanda NC, Singh V, et al. Live three-dimensional echocardiography of the human fetus. Echocardiography 2003;20:715—21. [23] Cognet T, Seguela PE, Thomson E, et al. Assessment of valvular surfaces in children with a congenital bicuspid aortic valve: preliminary three-dimensional echocardiographic study. Arch Cardiovasc Dis 2013;106:295—302. [24] Shen O, Yagel S. The added value of 3D/4D ultrasound imaging in fetal cardiology: has the promise been fulfilled? Ultrasound Obstet Gynecol 2010;35:260—2.