Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
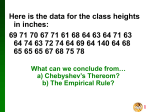
THE ASSESSMENT OF DECISION MAKING CAPACITY AFTER ACQUIRED BRAIN INJURY: LEGAL AND NEUROPSYCHOLOGICAL PERSPECTIVES June 29, 2015 Who We Were… Who We Are… Madeline DiPasquale, PhD Clinical Neuropsychologist Supervisor, Ambulatory Programs MossRehab- Drucker Brain Injury Center Tony Baratta, Esquire Attorney Baratta, Russell, and Baratta Goals and Objectives Define and distinguish between the terms competency and capacity. Understand the legal procedure to obtain guardianship and fulfill legal responsibilities to the Court thereafter Determine three cognitive and functional constructs evaluated as part of a capacity evaluation. Identify three evaluation methods used to help determine capacity. Determine if guardianship proceedings are appropriate. Identify two indicators for proceeding with guardianship and two steps in the process for obtaining guardianship. Why Discuss This Topic? Unique neuropsychological issues after brain injury Definitions of Terms Definition of Terms Power of Attorney Springing Power of Attorney Health Care Directive/Living Will Guardianship Health-Care Decision Making Pennsylvania Act 169 The Elements of Health Care Decision-Making ● Pennsylvania Act 169 designed to address end of life decisions (this is NOT GUARDIANSHIP) ● Definitions of incompetence and competence define three critical elements in sound health care decision making: ● UNDERSTANDING the risks, benefits, and alternatives; ● An individual must be able to MAKE a decision; and ● COMMUNICATE the decision to any other person(with technical assistance). ● If the ability to perform any of these decision elements is absent, the individual is incompetent to make that specific decision. When all three are present, the person is competent and his choice should be respected. ● Decision-making can be transient – competent to make some decisions but not others Health Care Agents and Representatives ● A health care power of attorney may vest an agent with authority even when the patient is competent (designated before change in health status) ● A health care representative may make health care decisions for an incompetent adult patient who has no controlling living will, healthcare power of attorney, or guardian of the person (after change in health status) Healthcare Agents and Representatives ●Unless a patient designated otherwise, the patient’s health care representative will be determined by a statutory list that generally gives priority in the following order: ● Spouse and adult child who is not the child of the spouse ● Adult child ● Parent ● Adult sibling ● Adult grandchild ● Close friend Guardianship This is serious business… ●“Determination of incompetence represents one of the most profound infringements of a citizen’s rights” (Grisso and Applebaum, 1998) Competency and Capacity: Complimentary Terms Competency Capacity ● Competency is a legal ● Capacity is what we construct ● Competency is always assumed unless proven otherwise assess ● It relates to a person’s ability to perform their life role ● “Right to folly”- people have the right to make a bad decision What We Do: Risk Assessment What’s the risk/benefit to the person making the decision? Areas for Determining Capacity ● Testamentary ● Donative ● Contractual ● Convey Real Property ● Execute a Durable Power of Attorney ● Consent to medical care ● Execute an Advance Directive ● Consent to sexual relations ● Capacity to drive Guardianship Petitions Two Main Areas for Guardianship ● Capacity to make decisions about your own personal protection: ● Protection of person ● Protection of the estate The Process for Appointing a Guardian Filing a petition Serving and explaining the petition Appointment of an attorney for the person with brain injury Hearing before an Orphans Court Judge Evidence presented Judge issues an Order The Neuropsychological Assessment of Capacity What Do We Evaluate When We Assess Risk? Understanding: the ability to understand diagnostic and treatment information Appreciation: relate treatment information to one’s own situation Reasoning: to rationally evaluate treatment alternatives, comparing risks and benefits and their impact Expressing a choice: communicating a decision The CEO of SELF The Neuropsychological Assessment of Capacity ● The assessment should always consider: ●Medical Condition ●Cognitive Functioning ●Daily Functioning The Neuropsychological Assessment of Capacity ●Values ●Social history ●Family history ●Cultural background The Neuropsychological Assessment of Capacity ●Risk of harm ●Level of supervision ●Means to enhance capacity How to Assess Capacity ● What’s the question? ● The evaluation must be tailored to answer the question for a specific capacity: finances, medical decision-making, etc. ● Review of legal standards ● What are the State’s requirements for determining capacity? ● Does the Court have any specific requests? How To Assess Capacity ●Clinical Interview ● Patient, family members, guardians ●Standardized Assessments ● Measures of orientation, intellectual functioning, attention, working memory, learning and memory, language skills, visuo-spatial skills, motor skills, executive functioning, emotional functioning ●Functional Assessments ● Bill paying, medication management, making appointments, route finding, household management Neuropsychological and Cognitive Constructs to Assess for Capacity and Competence ● Effort/Symptom validity ● Emotional functioning ● Intellectual functioning ● Attention and concentration ● Verbal skills and language ● Learning and memory ● Non-verbal/visuospatial skills ● Executive functioning ● Motor skills Standardized Assessment Tools ●Symptom and Performance Validity ●Intellectual functioning and academic achievement ●Attention, concentration, and working memory ●Visual-spatial skills ●Language processing ●Learning and memory ●Motor functioning ●Executive functioning ●Emotional functioning Functional Assessments Route Finding/Functional Mobility Task Medication Management Task Family Schedule Personal Business and Finance Task Situational Problem Solving Scenarios Example: Situational Problem Solving You get a phone call from a travel agency that tells you that you have won a free vacation to the Bahamas, for 3 nights and 4 days. All that you have to do is listen to a 2 hour promotional presentation and respond to a questionnaire. It will only cost you the taxes and shipping and handling for your promotional video and your vacation package, which comes out to $124.99. Do you accept this offer and pay the fee? Why or why not? Currently Available Standardized Functional Assessments Texas Functional Living Scale UCSD Performance-Based Skills Assessment Social Skills Performance Assessment Medication Management Ability Assessment Executive Function Performance Test MacArthur Competence Assessment Tool for Treatment The MacArthur Competence Assessment ToolTreatment (MacCAT-T) ● Utilizes a structured interview to assess the four legal standards (Understanding, Appreciation, Reasoning, Expressing a Choice) ● Assesses decision making abilities relative for judgments about patients’ competence to consent to treatment. The MacArthur Competence Assessment ToolTreatment (MacCAT-T) Responsibilities of the Clinician: ● Diagnosis and its features of diagnosis ● Disease course ● Recommended treatment ● Features of recommended treatment ● Benefits and risks of recommended treatment ● Alternative treatments The MacArthur Competence Assessment ToolTreatment (MacCAT-T) ● Disclose- Clinician describes the disorder and features ● Inquire- What do they understand about the information you presented? ● Probe- If any information is omitted or incorrect during inquiry, discuss and review ● Re-Disclose and Re-Inquire- Explain and review again, especially if patient’s omits or misunderstands Case Examples Case 1: Injury History ● 35 year old AA male injured 10.10.2011 as the result of a fall of 20 to 30 feet from a cherrypicker. After the fall the unit collapsed onto the patient. ● Neuroradiological studies identified subarachnoid hemorrhage, intraventricular hemorrhage, right superior frontal gyrus contusion, and diffuse axonal injury. C4-5 central disc protrusion, non-displaced L5 transverse process, and hip fractures ● Course of inpatient acute brain injury rehabilitation and outpatient services Injury History Continued ●Has been living at home. Recently admitted to inpatient, episode of violence on 9.9.2014. Restraining order in place. Referred for residential brain injury rehab- patient does not want to go ●Wife is current guardian of person and finances. Patient believes he is able to manage his own decisions and was particularly emphatic that he can manage his own finances ●Medications: Omeprazle (40mg/day), Abilify (2mg/day), Risperdal, 1mg/day), Lithium (450mg/day), Buspirone (12mg, Q12) Case 1: Social History ● Married with two children (married after injury) ● Wife is guardian of person and finances ● History of substance misuse (premorbid and post- injury) ● Currently driving (illegally) ● Episode of violence in home with arrest ● Agitation and anger Social History Continued ● History of placement in “home for boys” at age 13 ● Sexually assaulted Questions for the Evaluation ● The client wants to be his own guardian ● Can he make his own medical decisions? ● Can he manage his finances? ● Is he safe in his own home? Is his family safe with him at home? Evaluation Methods and Tools ● 4 hours to complete evaluation ● Records review ● Clinical interview ● MacCAT-T ● Personality Assessment Inventory ● Repeatable Battery for Neuropsychological Assessment (RBANS-Form B) ● Trails A and B ● Wisconsin Card Sorting Test A Quick Statistics Lesson Test Findings ● Trials A and B: 1st percentile ● Wisconsin Card Sorting Test: ● Maintain Mental Set: 1st percentile ● Categories Complete (2): 2-5th percentile ● Perseverative Errors : 1st percentile ● Non-perseverative errors: 23rd percentile ● Total Errors: 6th percentile ● Conceptual Level Responses: 9th percentile Emotional Functioning ● Evidence of positive impression management ● Denied any history or issue with alcohol or substance misuse ● “Two blunts per day, but I’m no weed head” ● Expansive mood, hostile and irritable ● Impulsive, resentful, high energy ● May meet criteria for mania or hypomania ● Inflated sense of self-esteem, grandiose, delusional beliefs o special skills ● Risk taker Results: RBANS Cognitive Domain Percentile Range Immediate Memory <1st Profoundly Impaired Visuospatial/ Construcitonal 2nd Profoundly Impaired Language <1st Profoundly Impaired Attention <1st Profoundly Impaired Delayed Memory <1st Profoundly Impaired Total Score <1st Profoundly Impaired Results: MacCAT-T Disclosure Patient Response Diagnosis: Traumatic Brain Injury “I have none of these symptoms” Feature of Disorder: • Impaired attention • Impaired learning and memory “I may forget some things, but I never forget about money. I walk around the house and see the lights on and remember to pay the light bill. I pay the gas bill because I want to drive my car. I sit around the house all day – that’s my problem.” Feature of Disorder • Impulsivity (substance misuse and spending) “No” Feature of Disorder: • Behavioral dis-control • Anger outbursts • Threats to others “No changes. It something bothers me and I get the chance I speak my mind. But I don’t get mad.” Course of Disorder: Treatment/Improvement “If I get intense therapy my left side will improve so I can run and play football with my son and patty cake with my daughter.” No Treatment “Won’t do me no good.” Recommendations ● Patient continues to require a legal guardian to support his safety, to make decisions for him, and to manage his finances. The court should be informed that patient’s relationship with his wife is strained (there is a restraining order in place as a result of his actions in the home on September 9, 2014). ●Patient will require ongoing pharmacological management and review of behaviors in association with medication changes. Recommendations Continued ●Patient would benefit from using goal-setting language (with clearly delineated tasks and aims) to support his overall goal of becoming his own guardian. It will be important for future clinicians to recognize this primary goal, and use this goal to support the reasoning behind all future treatments (emotional, physical, cognitive, and behavioral). While it is certainly unclear as to whether patient will ever achieve his desired outcome, using that goal for his “buy-in” to treatment will be critical. Recommendations Continued ●Patient has severe cognitive, emotional, behavioral, physical, and psychological deficits resulting from his severe traumatic brain injury. His personality style, combined with the cognitive, emotional, and psychological issues related to his brain injury, will directly impact his ability to develop and implement strategies to support his recovery. A neuropsychologist with extensive experience in working with persons with traumatic brain injuries would best serve to address these issues and to direct a treatment team on how to establish a relationship and implement strategies. Case 2: History ● 65 year old woman who was born in Guatemala and immigrated to the United States in the “1980’s” ● History of migraine headaches, without aura, hypertension, hyperlipidemia, asthma, macular degeneration, colonic polyps, gastric ulcer ● October 2003, experienced an episode of left arm numbness and weakness with pain. MRI reported as WNL ● Between 1995 and 2009, several episodes of dizziness, described as “lightheadedness” and “vertigo” ● Cardiac and neurological investigations into the possible causes of these episodes were negative. A CT scan in July 2007, following an episode, was reported as within normal limits History Continued ●July 2007, patient fell on a wet floor ● Loss of consciousness ● An additional thirty minutes of disorientation and complained of headache after the fall. Screening laboratory tests and CT scans of the head, cervical, and lumbosacral spine were negative, although degenerative facet hypertrophy was noted at L5-S1. Two findings were noted during the course of the July 2007 hospitalization: an EKG identified lateral ST depression, and bilateral leg tremors. History Continued ● Neurological follow-up July 2007 ●Diagnosed with idiopathic Parkinson’s disease, stage I: left arm dystonia, resting tremor of the left leg, mild cogwheel rigidity in the left arm, mild left deltoid and hip flexor weakness, mild left hypokensia, and bradykinesia. ●Mirapex (symptoms of headache and lightheadedness) ●Requip, which she continues on as of the writing of this report History Continued ●January 2009, pedestrian struck by a bus while crossing the street ● Altered state of consciousness and lying on her left side. She was disorientated, and with a Glasgow Coma Scale score of 13 ● CT findings: linear skull fracture, hyperactyte left temperoparietal subdural hematoma, significant mass effect from the subdural hematoma, and subarachnoid hemorrhages in both the Sylvian Fissure and high convexity. ● Emergency evacuation of the hematoma History Continued ● Two weeks acute care ● Confused and agitated, and required physical restraints to assure her safety so she would not fall. ● Acute brain injury rehabilitation from February 13, 2009 until March 5, 2009. ● Enclosed bed system for safety. ● Impulsive, misused familiar objects, and had decreased problem solving; she was unable to make medical decisions. ● Required 24/7 supervision to assure her safety, and to assist her in activities of daily living. ● In March 2009, the Court determined patient to be totally incapacitated, when her son and attorney appointed guardian of the estate, husband and daughter co-guardians of her person. ● Currently lives with husband, daughter (husband and 3 children) Social History ● Lives with husband, daughter, and daughter’s family ● Daughter is currently Guardian of the person ● Son is currently Guardian of the estate ● Prior to the 2009 brain injury, patient had amassed approximately $60,000 in credit card debt ● Following the January 2009 brain injury, acquired an additional $30,000 in debt Questions to be Addressed ● What are client’s functional performance strengths and limitations? ● Can the client understand the nature of her condition? Does she understand her financial and medical situations? ● Can patient weigh the risks, benefits, and consequences of her decisions? ● What is the recommendation to the Court regarding capacity to make her own medical and financial decisions? Evaluation: Standardized Measures ● The Montreal Cognitive Assessment (MOCA)- Spanish version ● Brown-Peterson Task: Consonant Trigrams (administered in Spanish) ● Grip Strength Test ● Wechsler Adult Intelligence Scale-IV: Comprehension Subtest (administered in Spanish) ● Ruff 2&7 Selective Attention Test ● Ruff Figural Fluency Test ● Wisconsin Card Sorting Test (administered in Spanish) Functional Evaluation ● Route Finding/Functional Mobility Task ● Utilize written directions to each location within the hospital. Given a list of 5 questions to answer at each location. This task requires attention to detail, environmental cues, problem solving, physical strength and endurance ● Medication Management Task ● Required patient to prepare 3 levels of prescriptions orders, using written instructions and bottles of “medications.” Task increases in demand, with prescriptions becoming increasingly more complicated. Required fine-motor skill, attention to detail and organization. ● Family Schedule ● Organize approximately fifty tasks for 4 family members across a week, given various events and parameters. Required attention to detail and problem solving, and planning and organization. She is given a weekly schedule/calendar and sticky notes to complete the task. Functional Evaluation ●Personal ● Business and Finance Task: cash version Given budget and food stamps amount. She was required to assign money from her budget to pay eight bills and to cover the cost of cost of additional food. Required problem solving skills, organization, and basic math skills. ●Situational ● Problem Solving Scenarios Presented with seven problem solving scenarios related to personal safety, social relationships, and financial decisions. Required reasoning, planning, problem solving, and judgment. Understanding Results Functional Performance Findings Strengths Activity Pattern Attention to Task Communication Skills Emotional Adjustment Functional Math Skills Physical Safety Awareness Use of Strategies Variable Skills Limitations Awareness of Attention to Detail Deficits/Insight into Problem Solving Disability Following Directions Physical Functioning and Endurance Planning and Organization Learning and Memory Rate of Performance Standardized Results ● MOCA 24/30 (Impaired) ● Brown Peterson : <1st percentile, profound impairment ● Ruff 2&7: ● Total Speed, 14th percentile (LA) ● Total Accuracy, 50th percentile (AVG) ● Comprehension (WAIS-IV): 9th percentile (LA) ● WCST4/6 categories completed 33 trials to complete first sort ● Grip Strength ● RIGHT: 2nd percentile (borderline) ● LEFT: 1st percentile (severely impaired) Recommendations to the Court ● At this time, it is my opinion, within a reasonable degree of neuropsychological certainty, that patient is not able to weigh the risks, benefits, and consequences of her financial decisions. It is my opinion, within a reasonable degree of neuropsychological certainly, that the financial guardianship remains in place. ● It is my opinion, within a reasonable degree of neuropsychological certainty, that patient can make her own medical decisions and be guardian of her person. Almost there… When and Why to Contact an Attorney ● Now, to decide while healthy who will make decisions for you if you cannot ● Immediately after brain injury: Guardianship if necessary or to ensure wishes set forth in Power of Attorney honored To guide family in medical decision-making regarding treatment To preserve evidence and fight to get back what is lost (wages, medical costs, loss of life’s pleasures, etc.) if injured due to negligence of another When and Why to Contact a Neuropsychologist Assessment of function developmental evaluation post neurological event Question of capacity Return to school Return to work Request for accommodations Change in mental status Very close now… Questions and Comments? Thank You!