Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
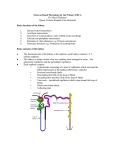
Lecture 13: Renal Physiology • Does your GI tract absorb into blood all nutrients? ions? water? 1. Now imagine that you drink water: 1 glass, 2, 3, 4, 5 glasses (1L). Does the additional 1 liter of water stay inside the blood vessels (18% increase of volume from 5.5L)? – No. Water will leak into interstitial fluid, so that the load will be redistributed between the vascular system and the tissues. One becomes 1kg heavier but blood volume is not affected significantly. 2. Now imagine that you drink isosmotic fluid: 300mOsm NaCl (one soup spoon of table salt per liter of water). Does the GI absorb all the ions? water? Does the additional liter of water stay inside the blood vessels? – Yes. Salt will not leave the blood vessels since there is no concentration gradient between the blood and extracellular fluid. Water will stay with salt, i.e. in blood vessels. One becomes 1kg heavier and blood volume is increased by 18% (assuming no kidney function). 3. Recall that after losing 1L of blood, arterial blood pressure (Pa) is decreased so much that one can collapse (blood donation = 0.5L). Would you collapse if you drink 1L of Gatorade? – No. Because kidneys can normally transfer extra salt and water into the bladder as fast as we drink and absorb it. • Kidneys receive 1 L/min = 20% of cardiac output at rest. • 20% of this volume (i.e. 200 mL/min = a glass of water/min) is filtered into the internal kidney tubules and, if necessary, kidney would dispose almost all of this amount into the bladder. Homeostasis of ions and water feedback control Kidney processes: 1. Filtration 2. Reabsorption 3. Secretion [H+], [Na+], [K+], blood volume=const controlled variables Sensors in kidney and elsewhere • • • Normal plasma Na+ levels: 135 to 145 • mmol/L. Very low Na+ (less than 125 mmol/L) • nausea, vomiting, headache, short-term memory loss, confusion, lethargy, fatigue, loss of appetite, irritability, muscle weakness, muscle cramps, seizures, • decreased consciousness or coma. Very high Na+ (greater than 157 mmol/L) seizures and coma. Normal plasma K+ levels: 3.5 to 5.0 mmol/L (98% of K+ is inside cells). Very low K+ (less than 3 mmol/L) muscle weakness, muscle pain, tremor, muscle cramps, constipation; flaccid paralysis and hyporeflexia. Very high K+ is a medical emergency due to the risk of potentially fatal abnormal heart rhythms. • Kidney is a waterproof bag with one high pressure tube in (==renal artery) and two low pressure tubes out (==renal vein and ureter) ultrafiltrate 1 Out In urine 2 3 urine is ultrafiltrate of blood from which nutrients and necessary ions were removed In kidney there are three processes: 1. Filtration: Blood ultrafiltrate is pushed into renal tubes. 2. Reabsorption: All glucose, all a.a. and necessary amount of ions are reabsorbed back into blood. Whatever left is excreted as urine. 3. Secretion: some substances are actively secreted into urine. Is everything that is filtered excreted? Was everything that excreted filtered? cortex • The building blocks of kidney are called nephrons from G. nephros=kidney • ~1,000,000 nephrons in each kidney are organized radially from medulla to cortex Renal tubule medulla Starts with renal corpuscle (initial filtering component) = a glomerulus + a Bowman's capsule Ends with collecting duct 2 1 Renal corpuscle Glomerular capillaries 4 3 5 ultrafiltrate Process 1: Filtration • renal artery 3 subdivides to form afferent arterioles 4 • Afferent arteriole subdivides into a smaller number of very short capillaries called glomerular capillaries 5 • The tuft formed of capillary loops is called glomerulus Glomerular capillaries Capillary types Glomerular capillaries Fenestrations ~ 60 nm wide • Glomerular capillaries are very leaky. • All substances smaller than 40nm can leave glomerular capillaries and go into Bowman’s capsule (the initial part of kidney tubules). • What substances are smaller than 40nm? 40nm RBC (7.5µm) human nail human hair thickness thickness (40-140µm) = 1mm (millimeter) ovum (140µm) = 1µm (micrometer) WBC (10-12µm) Neurons (10-20µm) axon diameter (1µm) = 1nm (nanometer) synaptic vesicle diameter (0.05µm) • where on this scale is human nail thickness? human hair thickness? RBC? neuron size? axon diameter? synaptic vesicle? thrombocytes Scanning electron micrograph of T lymphocyte (right), a platelet a.k.a thrombocyte (thromb- + cyte, "blood clot cell")(center) and a red blood cell Capillary types Fenestrations ~ 60 nm wide Glomerular capillaries • RBC (7.5µm) are not filtered • Glucose, a.a., ions, waste products including urea are filtered into Bowman’s capsule • What about proteins that are smaller than 40nm? (Albumin=lipid carrier, part of lipoprotein; Globulins=clotting factors, peptide hormone carriers, antibodies; Fibrinogen=blood clotting) • You do not want to loose proteins circulating in blood into kidney tubules. • How would YOU change morphology to keep proteins inside capillaries? Specializations of glomerular capillaries aimed to reduce protein filtration Efferent arteriole • Capillaries are covered by podocyte cells. • Podocyte cells have a number of protruding foot processes. • Space between foot processes makes filtration slits. Podocyte cells with protruding foot processes. Filtration slits make a sieve. Glomerular capillaries width of filtration slits ~ 40 nm - - - - - - - - • Filtration slits make a sieve that prevents molecules larger than 8nm to escape into kidney tubules. • In addition, podocytes are negatively charged and proteins are also negatively charged so that podocytes repel proteins that further reduces the ability of proteins to escape into kidney tubules. • Conclusion: very small filtration of proteins, even when proteins are smaller than 8nm 2 Space inside Bowman’s capsule 1 capillary podocyte 1 capillary 1 capillary red blood cell • • • • F = endothelial lining is highly fenestrated (F). P = podocytes extend primary processes (P1) that give rise to numerous foot processes (P2) FS = filtration slits The system is very efficient. E.g. serum albumin (steroid hormone carrier) has 3.55nm molecular radius. Less than 1% is filtered into renal tubules 2 1 Renal corpuscle or 200 L/day ultrafiltrate Glomerular capillaries 4 3 5 • Filtration summary: • 200mL/min = 200 L/day is filtered into the internal kidney tubules • Filtered: glucose, a.a., ions, waste products including urea • NOT filtered: RBC, most molecules bigger than 8nm, most proteins 120 L/day in proximal tubule 5 3 200 L/day Renal corpuscle or ultrafiltrate 2 Glomerular capillaries 1 6 4 Process 2. Reabsorption: • the renal tubule is continuous with Bowman’s capsule. • The epithelial cells of the tubule wall differ in composition and function along the tubule: • Segments: –3 Proximal convoluted tubule –4 Loop of Henle –5 Distal convoluted tubule –6 Collecting duct Reabsorption mechanism: 1. a.a.: co-transport with Na+ on luminal side, facilitated diffusion on blood vessel side 2. glucose: same ultrafiltrate • a.a. reabsorption cannot be saturated. • normally all glucose is reabsorbed. In diabetes blood [glucose] is so high that the absorption mechanism is saturated not all glucose is reabsorbed some glucose ends up in urine • Urea is not reabsorbed at all • Substances NOT regulated by kidney: – a.a. and glucose (reabsorb all) – urea (excrete all) – (NB: absorption is NOT regulation!!!) K+ 2 • Substances regulated by kidney: Amino acids 1 Amino acids Amino acids – Na+ (reabsorb only as much as necessary) – K+ (reabsorb only as much as necessary) – H+ (reabsorb only as much as necessary) – H2O (reabsorb only as much as necessary) • We will look at regulation of Na+ and H2O 120 L/day in proximal tubule 1 Renal corpuscle or 70% 200 L/day Na+ ultrafiltrate Na+ 2 30% Na+ 3 4 • 2.1 Regulation of Na+ • Bulk active reabsorption in the proximal 1 convoluted tubule (70%): co-transport with Glucose and a.a. • Fine Na+ regulation in distal convoluted tubule 2 and collecting duct 3 (30%) 120 L/day in proximal tubule 200 L/day Na+ 2 channels • 2.1 Fine tuning of Na+ reabsorption in distal convoluted tubule and collecting duct include regulation of: Na+ K+ ultrafiltrate 1 1. number of Na+-K+ pumps 1 2. number of Na+ channels on luminal membrane 2 Amino acids Amino acids • Both are regulated by Aldosterone 2.1.1 Na+ reabsorption: Aldosterone • Aldosterone is a steroid hormone produced by adrenal gland (steroid hormones act on nucleus to promote or inhibit protein production). • Aldosterone increases synthesis of Na+-K+ pumps and Na+ channels in the cells of distal convoluted tubules and collecting duct. • Aldosterone absent 2% of filtered Na+ is not reabsorbed but excreted. Na+ 2 channels • This is equivalent to 35g of NaCl Na+ per day • High Aldosterone almost all Na+ is reabsorbed • Eat high Na+ diet low Aldosterone • Eat low Na+ diet high AldosteroneAmino acids • What regulates Aldosterone? K+ 1 2.1.1 What regulates Aldosterone? • Aldosterone secretion by adrenal gland is directly stimulated by a hormone Angiotensin II. 1 Liver secretes Angiotensinogen into blood stream, so that Angiotensinogen is in high and stable concentration 3 Small polypeptide Angiotensin I (“A I”) is cleaved by Renin AI Angiotensinogen Angiotensin Converting Enzyme A II Renin is an enzyme 2 Na+ Depending on needs, Kidney (juxtaglomerular cells) release Renin into blood stream. 4 A I is converted into A II by angiotensin converting enzyme (ACE) on the luminal surface of capillaries particularly in the lungs • ↑Renin ↑A II ↑ Aldosterone ↑ #Na+ channels and ↑ #Na-K pump ↑ Na+ reabsorption • Thus: ↑Renin ↑ Na+ reabsorption ↑Pa • Renin is released by juxtaglomerular cells: Renal corpuscle 2 • How is Renin release regulated? 1 • Three inputs to juxtaglomerular cells: 1. SNS (external regulations): fight-or-flight ↑SNS ↑Renin ↑ Na+ reabsorption ↑ Pa 2. Juxtaglomerular cells function as baroreceptors: if ↓Pa ↓P 3 part of distal convoluted tubule in afferent arteriole ↑Renin ↑Na+ reabsorption ↑Pa Kidney 3. Osmoreceptors in macula densa located near the start of distal internal convoluted tubule. Macula regulation densa senses [Na+] in the tubular fluid flowing past it: ↓[Na+] ↑Renin ↑Na+ reabsorption 2.1.1 Renin / A II / Aldosterone • In addition, Angiotensin II is a potent constrictor of arterioles all over the body: • ↓Pa ↑Renin ↑A II constriction of arterioles ↑Pa ↑Aldosterone ↑Na+ ↑Pa • If Angiotensin II levels are continuously elevated, it could be one cause of hypertension. • Why continuous hypertension is bad? • What is the first line of defense against high blood pressure? • ACE inhibitors (angiotensin converting enzyme inhibitors): lisinopril, benazepril, captopril… 2.1.2 Atrial Natriuretic Factor (ANF) • ANF (small 28 a.a. peptide) is secreted by the cells of cardiac atria in response to distention which would result from increase of blood volume. 1. ANF is a powerful vasodilator 2. ANF acts on the distal convoluted tubule and collecting duct to inhibit Na+ reabsorption ↓blood volume 3. ANF acts on renal blood vessels to increase filtration (dilates afferent arterioles and constricts efferent arterioles) more blood plasma is filtered more Na+ can be excreted ↓blood volume ultrafiltrate 120 L/day in proximal tubule 1 Renal corpuscle or 70% 200 L/day Na+ ultrafiltrate Na+ 2 30% Na+ 3 4 • 2.1 Regulation of Na+ summary • Bulk active reabsorption in the proximal convoluted tubule (70%): cotransport with Glucose and a.a. • Fine Na+ regulation in distal convoluted tubule and collecting duct (30%): Renin A II Aldosterone, ANF 120 L/day in proximal tubule bulk1 Na reabsorption Renal corpuscle or 200 L/day + ultrafiltrate Na+ 2 fine Na tuning + 3 4 • 2.2 Regulation of water reabsorption • Bulk water reabsorption in the proximal 1 convoluted tubule. • Fine water regulation in the distal convoluted tubule2 and collecting duct 3 ultrafiltrate High osmolarity H2O K+ H2O Amino acids Amino acids Amino acids • 2.2.1 H2O bulk reabsorption • On the peritubular capillary side: – Na/K pump ↑Na+ – ↑[K+] due to K+ leaking back via K+ channels – ↑[glucose] – ↑[a.a.] • Increased osmolarity on the peritubular capillary side • Tight junction between cells of proximal tubule are leaky to H2O H2O leaks inside the kidney following osmolarity gradient and then into peritubular capillaries Case 1 Fluid inside collecting duct: 100 mOsm (a lot of water, very little salt) 100 mOsm ultrafiltrate H2O 100 mOsm H2O 100 mOsm a lot of water excreted into bladder medulla cortex Case 2 100 mOsm 300 mOsm 300 mOsm H2O 600 mOsm 600 mOsm H2O 1,200 mOsm 1,200 mOsm H2O medulla very little water excreted into bladder 2.2.2 H2O fine regulation in distal conv. tubule & collecting duct • Case 1. drink a lot of water: • distal convoluted tubule and collecting duct are generally impermeable to water water in not absorbed, but excreted. • Case 2. water needs to be conserved: • collecting duct becomes very leaky to water water leaks into kidney following osmolarity gradient and then into peritubular capillaries. • The permeability of collecting duct is regulated by insertion of water channels Lumen of the collecting duct Peritubular capillaries tight junctions High osmolarity Low osmolarity • The permeability of collecting duct is regulated by insertion of water channels • How water channels are regulated? • By antidiuretic hormone (ADH, also known as vasopressin) ADH • How is ADH regulated? • ADH is produced by a group of hypothalamic neurons and released from posterior pituitary ADH • ADH release is stimulated by: 1. ↓of firing of baroreceptors in atria and pulmonary vein 2. ↑ of blood osmolarity ↑of firing of hypothalamic osmoreceptors (they also generate the sense of thirst) • Why not position baroreceptors in aorta? • The receptors in aorta would measure Pa which does not change much; on the contrary blood pressure in atria and pulmonary veins is directly proportional to blood volume. • Case 1: Eat salty food ↑osmolarity ↑ADH ↑water reabsorption ↑blood volume ↓ blood osmolarity • Case 2: Hemorrhage ↓ blood volume ↓ firing of baroreceptors ↑ADH ↑water reabsorption ↑ blood volume 120 L/day in proximal tubule bulk1 Na reabsorption Renal corpuscle or 200 L/day + ultrafiltrate Na+ 2 fine Na tuning + 3 4 • 2.2 Regulation of water reabsorption summary • Bulk water reabsorption in the proximal convoluted tubule. • Fine water regulation in the distal convoluted tubule and collecting duct by ADH / water channels insertion • Let us come back to the example we have started with: • You drink a lot of isosmotic fluid (300mOsl = Gatorade) ↑ atreal baroreceptors firing GI absorbs all water and all salts ↓ ADH ↑ ANF ↓ H2O reabsorption ↑ blood volume ↓ SNS activity ↓ Juxtaglomerular cells firing ↑ filtration ↓ CO ↓ venomotor tone ↓ precapillary sphincter tone ↓ renin ↓A II ↓ Na+ reabsorption ↑ Na+ and H2O excretion: increased urine volume ultrafiltrate • You eat a lot of salt (e.g. salt-dried fish): movement of water from ICF ECF blood GI absorbs all salts ↑ blood osmolarity ↑ hypothalamic osmoreceptors firing ↑ osmoreceptors in macular densa ↑ ADH ↑ blood volume ↑ thirst ↓ renin ↓ Na+ reabsorption see previous slide Homeostasis of ions and water feedback control: regulatory mechanisms for Na+: renin, A I, A II, Aldosterone; ANF, ADH Kidney 1. Filtration 2. Reabsorption 3. Secretion [H+], [Na+], [K+], blood volume =const controlled variables I. Sensors: 1. SNS activity is function of Pa 2. baroreceptors function of Juxtaglomerular cells 3. osmoreceptors in macular densa 4. osmoreceptors in hypothalamus I. Sensors of blood volume: 1. in atria ANF 2. in atria and pulmonary vein ADH Thirst quenched right away • Your blood osmolarity is high and you feel thirsty. You • take a sip of water…. and you are not thirsty any more. • How does it work that you feel thirst quenched right away? It takes 20 minutes for water to get absorbed into blood. • “Thirst neurons anticipate the homeostatic consequences of eating and drinking, 2016”: the brain thirst neurons in subfornical organ are firing like crazy indicating that a mouse is really thirsty mouse takes a sip of water thirst neurons decrease firing. Another sip further reduction in firing. • Basically these neurons are measuring the difference between the amount of water needed and water that was consumed and update their firing rate in real time. • Zimmerman et al.:“thirst-promoting SFO [subfornical organ] neurons respond to inputs from the oral cavity during eating and drinking and then integrate these inputs with information about the composition of the blood. This integration allows SFO [subfornical organ] neurons to predict how ongoing food and water consumption will alter fluid balance in the future and then to adjust behaviour preemptively.” ultrafiltrate 1 2 3 Process 3. Active secretion into renal tubule (examples): – – – – H+ K+ Organic anions: choline, creatinine Foreign chemicals: penicillin • Properties: – Usually coupled to the reabsorption of Na+ – Primarily secretion occurs in the proximal convoluted tubule (except K+) – Secretion improves the efficiency of kidney to dispose of substances at a higher rate than the filtered load. Summary of kidney function • Major functions: • regulate water content • • Regulate ionic composition of K+, Na+, H+ NB: [H+] (in mM)=24PCO2/[HCO3-] (in nM); [HCO3-] is regulated by kidney • Excretion functions: • • • • • urea from proteins (Note that kidney does not regulate urea, kidneys just excrete all urea) uric acid from nucleic acids creatinine from muscle creatine creatinine bilirubin from Hb breakdown gives color to urine drugs, food additives, etc. • Endocrine functions: • • • erythropoietin (regulates RBC production) renin active form of vitamin D • During prolonged fasting: • kidney synthesize glucose from a.a. and release it to blood (gluconeogenesis). Kidney can supply as much glucose as liver at such times (done by cells of renal tubule). urine Nitrogen excretion • all animals have to excrete nitrogen waste from proteins degradation • Mammals excrete nitrogen as urea • Birds excrete nitrogen as solid uric acid • Excessive uric acid in blood of humans has been linked to gout, an inflammatory type of arthritis; and acute mania. Reducing uric acid improves symptoms. Guano • In the USA about 9% of the population has had a kidney stone. • The most common type of kidney stones contains calcium oxalate: • At 3 millimeters, stones can cause blockage of the ureter. This leads to pain, nausea, vomiting, fever, blood in the urine, pus in the urine, and painful urination. • Larger stones can block ureter completely and cause dilation of the kidney. • Formation: when urine contains more solutes than it can hold in solution, a seed crystal may form and grow. • Prevention: drink lots of fluids so that more than two liters of urine is produced per day, avoid soft drinks containing phosphoric acid (typically colas) Renal failure hemodialysis The principle: diffusion of solutes across a semipermeable membrane • What substances will you remove from blood? • What substances you don’t want to remove from blood? • stop here Table of permselectivity for different substances Substance Effective molecular radius (nm) Molecular mass conc. in ultrafiltrate / conc. in blood plasma sodium 23 0.1 1.0 potassium 39 0.14 1.0 chloride 35,5 0.18 1.0 water 18 0.15 1.0 urea 60 0.16 1.0 glucose 180 0.33 1.0 sucrose 342 0.44 1.0 polyethylene glycol 1.000 0.70 1.0 insulin 5.200 1.48 0.98 lysozyme 14.600 1.90 0.8 myoglobin 16.900 1.88 0.75 lactoglobulin 36.000 2.16 0.4 egg albumin 43.500 2.80 0.22 Bence Jones protein 44.000 2.77 1.0 hemoglobin 68.000 3.25 0.03 serum albumin (steroid hormone carrier) 69.000 3.55 <0.01 All proteins are reabsorbed via receptormediated endocytosis. Inside epithelial cells they are broken down into single a.a. which diffuse into blood Nucleotides filtration • • • • • • • • • • A nucleotide is a sugar, base, and phosphate. Nucleotides are molecules that, when joined, make up the individual structural units of the nucleic acids RNA and DNA. In addition, nucleotides participate in cellular signaling (cGMP and cAMP) Nucleosides are glycosylamines consisting of a nucleobase (often referred to as simply base) bound to a ribose or deoxyribose sugar via a beta-glycosidic linkage. Examples of nucleosides include cytidine, uridine, adenosine,guanosine, thymidine and inosine. Generally nucleosides are nucleotides (sugar covalently bonded to a nitrogenous base, such as adenine, guanine, cytosine...) that lack phosphates. However, for the sake of technical terminology, nucleotides are given classifications as nucleosides with a suffix describing the number of phosphates present in a specific unit. For example, if a nucleotide has one phosphate, it is a nucleoside monophosphate (NMP). If the nucleotide has two phosphates, then it is called a nucleoside diphosphate (NDP), and for three, it is a nucleoside triphosphate (NTP). The nucleotides that contain a ribose sugar are the monomers of RNA and those that contain a deoxyribose sugar compose DNA. GI: The GI tract digests nucleic acids into nucleotides, which are then digested by brush border nucleotidases into sugar, base and phosphate, which are then absorbed. Normal human should not have much in the way of free nucleotides in the blood. Kidney: 1. Yes, adenosine and the like are filtered and reabsorbed. Interestingly, in the "old days", we used to use the measurement of nephrogenous cAMP as an index of PTH activity (before we had good serum PTH assays). PTH stimulates proximal tubule phosphate excretion and distal tubular Ca reabsorption (as well as activating 1-OHase to convert 25D to 1,25D). 2. So here is the definite answer by a colleague who is both a nephrologist and a renal physiologist: Nucleotides are filtered and may also be secreted by the tubules. Much of them is known to be degraded within the tubular lumen. They may also act on tubular cells by binding to receptors on the apical membrane. Small proteins and peptides are reabsorbed mostly in the proximal tubule through endocytosis. 3. This is from Robert Unwin - an expert in this area to whom Eric Cohen (a nephrologist at MCW) referred the question. I agree with you Eric. Some debate about circulating levels of nucleotides, given content in rbcs, but our own data suggest very little ATP is filtered, so circulating levels of ATP at least must be very low. Less know about its breakdown products, including adenosine, but you might think it is higher. ATP can be measured in urine, but its source may be the bladder, rather than the kidney. Nucleotide cAMP Nucleoside Adenosine High blood pressure effect on kidney • High blood pressure can damage blood vessels in the kidneys, reducing their ability to work properly. • When the force of blood flow is high, blood vessels stretch so blood flows more easily. • Eventually, this stretching scars and weakens blood vessels throughout the body, including those in the kidneys.