Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
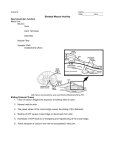
All muscles types: - 3 general functions of all muscle types: 1) motion 2) heat production 3) posture and body support - ALL muscles possess several basic properties, among them are: o Irritability—ability to respond o Contractibility—ability to shorten o Extensibility—once shortened it can return to own length o Elasticibility—one stretched it can return Skeletal Muscle Striated muscle - formation of skeletal muscle starts around the 4th week in utero from myoblast cells (nuclei pushed to the edge) - shortly before birth, myoblast production stops and all of the skeletal muscle cells that you will ever have are developed - there is NO hyperplasia of skeletal muscles cells after birth (there is hypertrophy—but never dev more cells) - the fleshy, thick, aka belly part of muscle—the gaster is almost always located on the bone proximal to the joint that the musc has an action on. - CT arranged in the muscle to strengthen, protect and binds muscle fibers together into whole muscle in a specific sequence that is to say, individual muscle fibers are surrounded by endomysium. The endomysium supports blood vessels and nerves to individual fibers - Groups of fibers are bound by perimysium into bundles, this supplies blood to the endomysium. And the entire muscle is coved by the epimysium, which is continuous with the tendons of the distal and proximal muscle. - These layers are continuous with each other. So: the Endomysium is attached and continuous with perimysium epimysium attached to tendon - *Critical to transmit the contractile forces from the cell to the tendon. - If there is a rip, it will reduce the force development transferred to tendon - Injury to CT tissue without injury to the contractile muscles CT diseases could effect movement even if the muscle is contracting properly. - Types of skeletal muscle: o Fusiform (long muscles, weaker), o convergent muscles (fibers converge at the point of insertion, ex, deltoid or pec major), o pennate muscles (strong muscles with high concentration of fibers per unit area, short in general and fatigue very easily, ex. Muscles in forearm), and o circular muscles (sphincters) - **Sliding Filament Theory*** review it, ***be able to DRAW a sarcomere, etc. Label the ZONES - Skeletal musc fibers are elongated cylindrical cells are unique because they are multinucleated and striated on a cellular level: o each cell is surrounded by a membrane called a sarcolemma, o within the muscle cell is sarcoplasm (is the cytoplasm of muscle cell), o from a functional standpoint, it has a network of membranous channel: sarcoplasmic reticulum o system of transverse tubules (T-tube), formed by narrow invaginations of the sarcolemma (cell membrane). These T-tubes run perpendicular to the sarcoplasmic reticulum, and the key impt is that these tubes are open to the extracellular fluid. o Embedded in the sarcoplasm and extending the entire length of the muscle fiber, are the myofibrils. Each myofibril is composed of myofilaments: thin (actin) and thick (myosin) filaments. o Arrangement of myofilaments is what gives the alternating light and dark bands o H zone—central region of the A-band. The A-band (at rest) contains thick and thin filaments o The I band—contains only thin filaments from adjacent sarcomeres and the midpoint of the I band is the Z line (Z line to Z line is one sarcomere), M-line (line down the middle of the central H band) Overview of the Sliding Filament::: Sliding of the filaments is due to the action of the cross bridges (extend out from the myosin toward the actin) Most impt at rest, the crossbridges on either side of the H zome are pointed in opp direction. The end of each cross-bridge terminates in a globular head and each globular head contains an ATPbinding site, which is closely associated with an myosin binding site on the actin. The globular heads function as a myosin-ATPase enzyme, splitting ATP into ADP +P, and these products with inorganic phosphate remain attached to their binding sites as their cross-bridges bind to the actin. This causes a conformational change. Conformational change—when cross bridges bind to the sites on the actin, 1) the ADP and P are released 2) crossbridges changed their orientation and rotate towards the center of the sarcomere shortening the distance betw the z-lines resulting in power stroke (pulling the z-lines together) 3) end of the power-stroke, each cross-bridge binds to a new ATP molecule which causes the cross bridge to release its hold on the actin. 4) 2 critical things to remember: 1- ***Splitting of ATP to ADP is necessary for cross-bridge and the actin to attached to each other and exert a power-stoke. *** Equally as impt is that the attachment of a fresh/new ATP is required for the cross-bridge to release its attachment to the actin at the end of the powerstroke. Rigor Mortis—stiffness post death. Regulation of cross-bridge attachment to actin is a function of: troponin and tropomyosin (two other regulatory proteins) - F actin is made up of several hundred fillaments of G actin which are strung together, formed in a double row and twisted to form a double helix - Tropomyosin lies in a groove betw the chains of F actin filaments - Attached to the tropomyasin is Troponin - Arrangement in resting musc (T-T complex = troponin and tropomyosin) - T-T complex worked together to control the cross bridges. At rest the T-T complex physically blocked by the active site of the actin filament, inorder for active site to be exposed, need Ca. - Calcium is stored in the sarcoplasmic reticulum of skeletal muscle, at relaxtion Ca concentration in sarcoplasm is very low, upon stimulation Ca concentration quickly rises in the sarcoplasm. That Ca binds to the troponin on the T-T complex, and moves it out of the way to expose the active site on to which the myosin crossbridge can attach - One the myosin crossbridge attaches, contraction takes place. As long as Ca stays bound and active actin sites exposed, the contraction will continue. - Contration is turned on when Ca binds to triponin and when the stimulus is removed, the Ca is actively pumped back into the sarcoplasmic reticulum for storage. (Skeletal musc is different because it STORES the Ca for use, in terminal cisternae. This terminal cisternae are seprerated by a narrow gap from the Ttubes) - - Action potentials from a motor neuron release acetylcholine, which open up gates to positive ions establishing an action potential on surface of muscle cell. This potential travels in both directions along the sarcolemea then down the T-tubes causing Ca released from the terminal cisternae. Ca bind to triponin, moving T-T complex out of the way, cross bridge attaches to active actin site, power stroke occurs following power stroke ATP and P released and new ATP attaches to crossbridge allowing to release grip on actin and jumps back to original position. ATP broken down and energy stored in crossbridge Review Neuromusckular system and terminology involved: -terminal end of motor neuron makes a junction approx at midpoint of a muscle fiber. At this point we have a junction, once an action potential crosses this junction it will travel in both directions along that muscle fiber. -The motor neuron, pushes in on the surface, invaginating the surface of muscle fiber but does not pierce the membrane. This indentation, called the synaptic trough. The space between the trough and the end of the motor neuron is the synaptic cleft. It’s across this cleft that acetylcholine must travel. -When the action potential reaches the end of the motor neuron, Ca ions enter the end of the motor neuron allowing acetylcholine to be released from small vesicles within the end of the motor neuron. -Without adequate Ca, acetylcholine release is depressed -within one millisecond of release, it is either diffused back into the motor neuron or is broken down by acetylcholinesterase -acetyl increase the permeability to positive ions -many drugs affect ACH Pathology - Myasthenia Gravis (MG)—autoimmune disorder that is associated with the destruction of the Ach receptors on skeletal muscle - Several drugs that have an effect that is similar to Ach, but the problem is that they are not destroyed by Ach-esterase - Among them, methylcholine, and carboxyl –same effect as Ach but are NOT destroyed—resulting in muscle spasm. Then there are curariform drugs (like curary) that compete with Ach sites thereby locking neuro-muscular junctions. Resulting in flaccid paralysis. The length-tension relationship - Strength of contration depends on thickness of fibers, muscle arcitecture and the initial length of fiber at rest - If fiber is at 100-120% of maximal length at rest can develop maximal tension - describes the amt of tension that can be developed by a sarcomere based on the distance from Z-line to Z-line before it is stimulated - if you take a sarcomere and decrease the distance from Z line to Z line to 60% of its normal resting length, it loses its ability to contract - if you were strong enough to pull (elongate) the sarcomere, 160-170% of its resting length, it also will no longer be able to contract - isometric contraction vs isotonic contraction - isometric: contraction of muscle, feel tension but no movement. At this point the muscles are contracting at a cellular level but tension is being absorbed by elastic components and is resisted by the weight of the load. (ie. Postoral muscles) - isotonic contraction: change in length but no change in tension - eccentric vs accentric - contraction is active and require ATP. ATP supply depends on availability of oxygen and organic energy sources like glucose and fatty acids. ATP can be produced both anarobically and arobic - - - anaerobic beneficial b/c not o2 dependent but is more limited in yielding ATP and results in production of lactic acid which is a major factor of muscle fatigue aerobic is o2 dependent results in more ATP production and doesn’t produce toxic end products immediate energy: derived from ATP and P groups stored in the muscle. Stored P groups are transferred to ADP to form ATP and this is enzyme dependent. Enzymes such as: Myokinase- transfer P from one ADP to another converting it to ATP and Creatine Kinase- obtains P from P storage molecule and donates it to ADP to make ATP but both of these only supply energy for a very short duration (6-10 sec up to 50-60 sec), depending on intensity of activity. As this is exhausted we switch source of ATP to aerobic production. Muscle fatigue: caused by glycogen depletion in muscles thereby decreasing ATP synthesis. The ATP shortage slows down action of NA-P pumps compromising membrane to maintain it’s resting potential which alters excitability of muscle. Lactic Acid production: decreases pH in sarcoplasm inhibiting activity of enzymes Loss of K ions with each action potential: Hyperpolarizes the cell making it less excitable Junctional fatigue: as ACH is depleted from the motor neurons Skeletal classified in fiber types: Type 1- slow twitch, red, oxidative fibers. They are well endowed with mitochondria and myoglobin. They have a high capillary concentration, hence their red color. They are well adapted for aerobic metabolism Type 11- fast twitch, white, glycolytic fibers. Adapted for quick responses. These are very rich in enzymes associated with phosphogen system for energy production. Their sarcoplasm releases and absorbs Ca very quickly. They have less mitochondria and myoglobin and less capillary concentration giving them their lighter appearance Type 2A fibers- are intermediate and have characteristics of both one and two. It’s believed that what we have in terms of percentage of each fiber type is dependent on genetics. This is why some people are born marathoners and others no matter how well they train may never become marathoners. SMOOTH MUSCLE: - except for the heart (made up cardiac mm) and skeletal mm - the muscle tissue in the walls of all hollow organs is smooth mm tissue o although the chemical and mechanical events of contraction are similar o smooth muscle does have several unique characteristics: smooth musc fibers are spindle shaped with 1 nucleus (centrally located) fibers are dramatically smaller lacks tough connective tissue sheathes around them a small amount of thin CT is secreted by the smooth mm cells themselves w/in this thin covering – blood vessels and nerves are found Most fibers are organized into two sheathes of closely opposed fibers running perpendicularly to one another The longitudinal fibers dilate and shorten the tube when they contract While the circulatory fibers, elongate and narrow a tube In the GI tract, when these fibers contract sequentially—results in peristalsis Contraction of smooth mm in the rectum, urinary bladder and uterus – help these organs expel their contents - Smooth musc DOES NOT HAVE, structured specific neural muscular junctions of skeletal mm o Instead: The innervating fibers (part of ANS) have numerous enlargements varicosities These varicosities release NT (neurotransmitter) into a wide synaptic cleft in the general area of smooth mm cells - Have much less organized sarcoplasmic retinaculum and NO T-tubes - - - - - - - Sarcrolemma has many invaginating pouches, which hold ECF with high Ca+ concentration right next to the membrane o As a result: When Ca+ channels open , large amounts of Ca+ from ECF enter the cell o Contraction ends when Ca+ ions pumped back out into ECF Has gap junctions that spread the impulse from cell to cell o (unlike skeletal mm) innervations occur as cells themselves act as pacemakers with unstable membrane potentials o Intensity and Rate of smooth mm contraction – can be modified by neural and chemical stimuli Mechanism of contraction: similar to skeletal o Myosin and Actin interact via sliding filaments o Process is energized by ATP and requires Ca+ ions o Smooth muscle has no striations and no sarcomeres It DOES have thick and thin filaments, but are much more longer and are chemically a little different than actin and myosin. Smooth musc has NO troponin and tropomyosin complex (T-T complex) o Difference: in smooth muscle During excitation contraction coupling, Ca+ ions activate myosin by interacting with a regulator molecule called: Calmodulin Calmodulin is a cytoplasmic Ca binding protein Interacts with Myosin Kinase enzyme, phosphoralating the myosin-like heads in smooth mm Thin filaments in smooth mm lack troponin Active sites are always exposed and always ready for contraction Relaxes when intracellular levels of Ca+ are decreased Some events that result in a decreased of Ca+ are due to: Detachment of Ca+ from calmodulin Actively transported into ECF Dephosphorylation of Myosin heads o Reducing the activity of myosin ATPase Smooth mm takes 30x longer to contract and relax than skeletal o **Smooth mm can maintain the same contractile tension for a prolonged period of time at less than 1% of the energy cost of skeletal muscle ATP contraction is extremely impt for overall body homeostasis o ** the smooth mm in small arterioles and other visceral organs, routinely maintain a moderate degree of contraction (smooth mm tone) Enough ATP is made via aerobic pathways to keep up with its demand The Neural response of Smooth Muscle to stimulation depends on the type of NT released and the receptors on that smooth mm: o All skeletal mm receives Ach at myneural mm o But different smooth mm has different receptors: Respond differently, sometimes to the same NT Ex: Bronchioles smooth muscle when exposed to Ach—causes bronchoconstriction, but when exposed to norepinephrine, a different group of receptors causes bronchodilation. But when the same norepinephrine attaches to vascular smooth mm—causes vasoconstriction. Some smooth mm layers have no nerve supply at all o Bc of transient membrane potential – depolarize spontaneously (or in response to chemical stimuli) Chemical Factors that cause smooth mm contraction or relaxation w/o an Action Potential do so by enhancing or inhibiting Ca+ entry into the sarcoplasm o Chemical Factors: Certain hormones Ex: Gastrin – hormone that increases smooth mm activity in stomach Hypoxia in smooth mm Histamine Hypercapia (high PCO2) Low pH MUSCLE METABOLISM Maintaining ATP supply: Creatinine – produced and secreted into blood stream from skeletal muscle at a fairly regular rate Freely filtered from body by kidneys and excreted in the urine (not reabsorbed) Creatinine serum level is a marker of renal function When a pt’s renal function is compromised, the GFR decreases and serum creatinine level rises The higher the serum creatinine level, the worse is the GFR Kidney function is routinely assessed in the clinical setting by reporting the pt’s baseline and current serum creatinine level Measurement of serum levels of CPK Distinct isoforms of CPK are found in diff. tissues Skeletal muscle = CPK-MM Elevated CPK-MM could indicate skeletal mm trauma or necrosis Ex: polymyocytis, rhabdomylysis Elevated CPK = MB is diagnostic for MI Cardiac Muscle = CPK-MB When one is damaged and cells are lysed, there is a release of tissue specific CPK isoforms from the cells into the blood Measurement allows for assessment of specific tissue damage Specific cardiac isoforms, regulatory molecules of troponin can be measured in the blood Troponin I and Troponin T Cardiac Troponin assays are very expensive and are routinely done in diagnosis in coronary syndromes and MI Pathologies associated with musculoskeletal system: Specific to abnormal NM junction function Myasthenia Gravis (MG)—autoimmune disorder that is associated with the destruction of the Ach receptors on skeletal muscle Exertional fatigue and weakness that is worse with activity and better at rest Attacks more females in the younger population, but 50+ = more males affected 25% of MG pts, thymic tumors are found Associated with destruction of the post-synaptic Ach receptors Results in diminished transmission of nerve impulse (NM junction) Muscle depolarization is incomplete or not achieved at all Myopathies: Muscle strength, tone and bulk are affected One of the most useful tests for mm function is the serum CK concentration CK used by muscle to convert creatine phosphocreatine (PC) – required for energy storage When muscle tissue is damaged, CK leaks into the serum EMG – Electromyogram Used to assess contractile status of a muscle as well as NM junction disorders Activity at a myoneural junction - skeletal musc has to be stimulate to contract - motor neuron stimulates, it brings the action potential to the myoneural junction - myneural junction = muscle—nerve junction - action potential from the motor neuron causes the release of acetylcholine from the endplate of the neuron. - Ach goes across the gap betw the neuron and musc cell membrane, where it causes the opening of Na+Channels on the musc membrane—creating an action potential on the muscle cell. That action potential is then traveled down the T-tubes initiating a contraction. - Ach has to be destroyed—by acetylcholinesterase.